
The Wernicke's aphasia, Sensory aphasia or receptive aphasia is a speech disorder in which the individual will have problems understanding the language heard, or repeating words or phrases that others have said; while the pronunciation will be correct.
Therefore, Wernicke's aphasia is the inability to understand words or to speak producing a coherent meaning, having preserved the articulation of speech sounds. In this way, there is a mutual lack of understanding between the patient and his interlocutor; having this to make a great effort to understand the affected.
When a patient with this problem arrives for consultation, his rapid and uncut speech is striking, which requires the other person to intervene to stop. In fact, the affected person does not usually realize that what he says does not make sense and they do not feel that there are problems in the dialogue (or attempted dialogue).
Article index
According to Luria, this disorder has three characteristics:
In other words, in order to properly listen and emit the sounds of speech, you must first know how to recognize the sounds in your own language. People with this problem are not able to isolate the characteristic sounds of their language and classify them as known phonemic systems.
He has no problems articulating speech, however, by confusing the phonetic characteristics, he produces the “word salad” (emitting words without connection to each other, giving rise to an incoherent speech, but without losing fluency).
As a consequence of the problem of poor recognition of phonemes, it will not be able to evoke graphemes (graphic representations of phonemes, like a written letter).
It can be acute (due to head trauma, stroke, neoplasms, etc.) or chronic (concomitant with Alzheimer's).
In Wernicke's aphasia, the affected areas are found in the parietal and temporal lobes of the dominant hemisphere (usually the left), the severity of the deficit depending on the magnitude of the lesion..
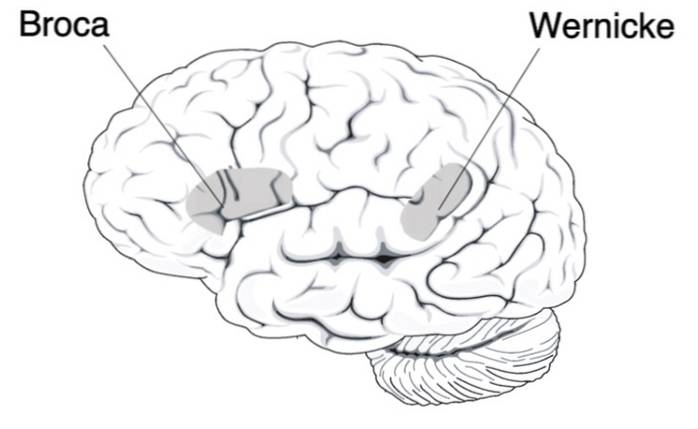
At first it was thought to be due to damage or malfunction in the Wernicke area, Where does your name come from. An area of the brain responsible for language comprehension processes, located in the posterior part of the temporal lobe of the dominant hemisphere (usually the left).
However, it appears that the key deficits in this type of aphasia are not only due to damage to that area; rather, it is somewhat more complex since:
It has then been suggested that the main difficulties in this disorder stem from damage to the medial temporal lobe and the underlying white matter. This area is adjacent to the auditory cortex.
Its appearance has also been seen by alterations in a certain part of the superior gyrus of the temporal lobe, affecting the connections with other nuclei responsible for language located in occipital, temporal and parietal regions..
On the other hand, if Wernicke's area is damaged, but in the non-dominant hemisphere (usually the right), aprosodia or dysprosodia will appear. This means that there are difficulties in capturing the tones, rhythm and emotional content of expressions of language..
This happens because the right hemisphere is generally in charge of regulating the understanding and production of speech, affecting the interpretation and emission of intonation and rhythm..
Wernicke's aphasia is usually due to a stroke, although it can also occur from blunt trauma due to an accident.
In conclusion, it is better to consider Wernicke's area as a very important area in this type of aphasia, forming part of a much broader process that includes more structures and their connections..
This type of aphasia can present in different ways and at different levels of severity. Some affected may not understand any spoken or written speech, while others may carry on a conversation.
The disease usually appears suddenly, while the symptoms appear little by little. The main symptoms of a person with Wernicke's aphasia are:
Problems understanding language, even single words or simple phrases. They may not even understand the sentences they say themselves. However, understanding can deteriorate in very different degrees and the patient will have to use extralinguistic cues (tone of voice, facial expression, gestures ...) to try to understand the other.
The affected person can understand several words or that a topic is being discussed, but only for a very short period of time. If you talk more than necessary, the patient cannot understand you; the problem increasing when there are other distractions such as noise or other conversations.
The stark contrast between fluent speech and the meaninglessness of the message is striking. They also emit phrases or sentences that are incoherent because they add non-existent or irrelevant words.
The level of errors they make in the expression of the speech of these patients can be variable, some can only have 10% errors while others 80%.
These are difficulties in choosing and organizing the letters or syllables of a word, or verbal paraphasias, in which a real word is substituted for another that is not part of the semantic field.
A common symptom is misinterpretation of the meaning of words, pictures, or gestures. In fact, colloquial expressions such as: "it is raining heavily" or "see all the color of rose" can be taken literally..
That is, they do not realize that they are using words that do not exist or that are not correct in that context. They do not know that what they say may not make sense to the recipient.
Interestingly, the words of the affective type or associated with emotions are preserved. Therefore, it seems that the words that are forgotten or replaced are those that do not have emotional content for the person, without depending so much on the meaning of the word itself.
Difficulties in repetition, reflecting their comprehension problems. Sometimes they add more words or phrases (this is called enlargement) or introduce made-up words or paraphasic distortions.
In some cases, mild neurological signs such as paresis on the face may appear, which are usually temporary. They can present cortical sensory problems, such as deficits in the recognition of objects by touch.
These symptoms, among others, are associated with the acute phase of the disease and resolve over time in parallel with recovery from brain injuries..
- Sometimes they string together a series of words that sound like a sentence, but together they don't make sense.
- Neologisms or invention of words.
- Anomia: Difficulty finding words.
- Change verb tenses, forget to say the keywords.
- In some cases, lack of pragmatic skills. They may not respect the turns of a conversation.
- Speech pressure or verbiage: excessive increase in spontaneous language, that is, the person does not realize that he is talking too much.
- Jergafasia: incomprehensible oral expression, due to the large number of parafasias they present.
- They have deficits in the naming of objects, animals or people; although they can do it with the help of the examiner (if he tells you, for example, the first syllable of the word).
- Reading and writing problems. Letter substitutions, rotations, and omissions occur when writing.
- Problems can be observed when performing simple gestures such as saying goodbye, asking for silence, throwing a kiss, combing hair ... which is a symptom of ideomotor apraxia.
- Copying of drawings with lack of detail or totally unstructured.
- Normal rhythm and prosody, maintaining proper intonation.
- They do not present any motor deficit, because as we said the articulation of speech is preserved.
- Intellectual abilities that are not related to language are completely preserved.
Here you can see what language is like in a patient with Wernicke's aphasia:
According to Rabadán Pardo, Sánchez López and Román Lapuente (2012) the types of Wernicke's aphasia depend on the extent of the lesion in the brain.
There are patients with small damage to the superior gyrus of the temporal lobe and others, however, also have lesions in nearby structures such as the subcortical white matter and the supramarginal and angular gyri. The latter will have the language much more damaged.
In this way, there are two types:
There is only damage in the Wernicke area. Many authors think that this is not a type of aphasia, since it only affects the reception of oral language and they classify it as a type of agnosia. These patients tend to understand written language better than oral.
Lesions in Wernicke's area and other adjacent areas. Not only are there difficulties in recognizing sounds, but there are also deficits in oral, gestural and written expression and comprehension.
It is not surprising that Wernicke's aphasia is not diagnosed correctly, as it is easy to confuse with other disorders. A differential diagnosis must first be made with a thorough neurological examination.
This is important because a bad diagnosis will have the consequence that the real problem is treated late or is not treated and thus the patient cannot improve..
Therefore, Wernicke's aphasia cannot be confused with psychotic disorder, since the way of expressing and behaving can be similar, such as incoherence of language or the appearance of disorganized thinking.
As each person presents the disorder differently, the treatment will depend on the affectation and severity that occurs. In addition, the existing treatments are varied.
The first 6 months are essential to improve language skills, so it is important to detect aphasia and intervene early. It is important because the cognitive alterations would stabilize in a year and after that time, it is difficult for the patient to improve significantly.
There is no definitive method that is always effective for Wernicke's aphasia. Rather, experts have focused on compensating for impaired functions.
Many times patients with aphasia do not demand treatment for themselves, because they are not aware that they have problems. In order to intervene, it would be very helpful if the person was first motivated by making them understand their deficits and inviting them to treatment. Thus, cooperation with therapy is facilitated and results are better.
These are the areas / aspects that are treated in Wernicke's aphasia:
First of all, we will try to improve patient communication. To do this, as soon as possible, they will be taught to communicate by means of signs, gestures, drawings or even using new technologies (as long as their damages are milder)..
Promoting strategies and skills for effective communication. They are framed in real contexts to facilitate understanding: such as ordering food in a restaurant, getting money at the cashier, going to the supermarket ...
The interlocutor should provide the patient with contextual clues, speak more slowly and in short sentences (and gradually increase the difficulty) and be redundant so that the patient understands better.
It intervenes outside the consultation, in a real environment. This encourages the patient to use the knowledge they had before the brain injury and use it to express themselves and understand others.
Above all, training the conserved capacities linked to the right cerebral hemisphere: understanding facial expressions, tone of voice, prosody, gestures, postures ... Semantic memory is also enhanced, which is the one referred to concepts and definitions.
Intervention to improve short-term memory and working memory has been found to be effective in Wernicke's aphasia. This is based on the fact that, repeating words increases their memorization, which helps to link them with their meaning, improving the understanding of sentences and making the person include them in their vocabulary.
Those who received this treatment increased the number of words remembered and even began to include verbs that had not been taught in the treatment.
The objective is to improve your attention to the auditory messages that come to you from others and from your own voice. It is very effective in treating verbiage as it teaches patients to listen carefully instead of speaking.
The specialist will give the patient certain instructions, using discriminative stimuli that he has to learn to identify (such as gestures or certain facial expressions). The affected person will end up associating these stimuli with stopping talking and starting to listen.
It is important that the affected person learns to slow down their own speech and supervise it.
Some authors consider it to be an effective treatment that works by increasing the activity of neurons in the affected areas. They defend that, in this way, brain reorganization is facilitated and; therefore, the recovery of language. It consists of subjecting the patient to strong, controlled, and intensive auditory stimulation.
In a study by Yoon, Kim, Kim & An (2015) a case is presented of a 53-year-old patient who received treatment with donepezil for 12 weeks, finding a significant improvement in language coupled with better brain recovery.
The help of the family is essential, introducing it in the treatment programs so that progress is better and faster. Thus, the specialists will educate the family so that they understand the disorder and stimulate the patient when and as necessary. Mainly they will be taught to adjust speech patterns to increase communication with the affected family member..
The prognosis of this disorder depends on the severity of the symptoms and the degree of impairment of listening comprehension; since the more affected it is, the more difficult it will be to recover normal language.



Yet No Comments