
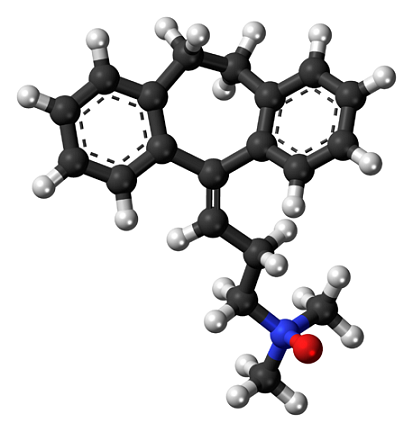
The tricyclic antidepressants (ADT) are one of the first antidepressant drugs discovered. Its name is due to its chemical structure, which is composed of three rings. They are effective in treating depression, although they are also used for other conditions such as bipolar disorder, panic disorder, obsessive-compulsive disorder, migraines or chronic pain.
The antidepressant effects of these drugs were discovered by accident, as previously only their antihistamine and sedative properties were known. Since this discovery, they have been the pharmacological treatment par excellence for more than 30 years. It began to be commercialized from the end of the 50's; and around the 80s, its use was reduced with the “boom” of selective serotonin reuptake inhibitors (SSRIs).
Currently they are prescribed less frequently; since they are being replaced by other antidepressants that cause fewer side effects. However, they can be a good option for some people when other treatments have failed..
Article index
It is believed that in individuals with depression there is an imbalance in certain brain chemicals called neurotransmitters. More specifically, it is associated with a deficiency of norepinephrine or serotonin.
There are several complex processes that can cause this neurotransmitter depletion. Antidepressants work on one or more of them with one goal: to make the levels of available norepinephrine, dopamine or serotonin rise to a safe point. This would result in the interruption of depressive symptoms.
Tricyclic antidepressants actually have five drugs in one: serotonin reuptake inhibitor, norepinephrine, anticholinergic and antimuscarinic drug, alpha 1 adrenergic antagonist and antihistamine.
The main mechanism of action of tricyclic antidepressants is the inhibition or blocking of the so-called “monoamine reuptake pump”. Within the monoamines, in this case we speak of serotonin and norepinephrine.
The reuptake pump is a protein that is located in the membranes of neurons (nerve cells in the brain). Its function is to "absorb" the serotonin and norepinephrine that have previously been released, for their subsequent degradation. Under normal conditions, it serves to control the amount of monoamines that are acting in our brain.
In the case of depression, as there is a small amount of these substances, it is not convenient for the reuptake pump to act. This is because it would decrease that amount even more. That is why the mission of tricyclic antidepressants is to block this reuptake pump. Thus, it works by increasing the levels of the aforementioned neurotransmitters.
However, what guarantees that the effects achieved with the antidepressant are maintained over time (even if it is stopped taking), is that this blockage produces changes in the brain.
When there is more serotonin or norepinephrine in the synaptic space (the one between two neurons that connect, exchanging information), the receptors responsible for capturing these substances are regulated.
In depression, the brain changes, developing many receptors for monoamines. Its objective is to compensate for the lack of these, although it is not very successful.
In contrast, tricyclic antidepressants increase monoamine levels at the synapse. The receptor neuron captures this increase, and its number of receptors decreases little by little; since you stop needing them.
Regardless, tricyclic antidepressants appear to be very effective for treating:
- Fibromyalgia.
- Pain.
- Migraines.
- Severe depression It seems that the greater the depression, the more effective this treatment is. In addition, it is more advisable in those people whose depression is endogenous, and with genetic components.
- Sedatives or hypnotics (for sleep).
Logically, this type of drug is not recommended for the following cases:
- Patients with poor tolerance to urinary retention, constipation, and daytime sedation.
- People with any heart disease.
- Overweight patients.
- Those who are at high risk of suicide. Since tricyclic antidepressants are toxic in overdose, and these patients can use them for this purpose.
- Patients taking several other medications at the same time, as unwanted drug interactions may occur.
- People with some dementia.
- Epileptic people, as it increases the frequency of seizures.
On the other hand, these drugs are usually discouraged for people under 18 years of age and can be dangerous in periods of pregnancy, lactation (since they pass into breast milk), if alcohol or other drugs, drugs or supplements are consumed..
Tricyclic antidepressants are administered orally and are rapidly absorbed from the gastrointestinal tract. They are very soluble in lipids, which gives rise to a wide and rapid distribution throughout the body.
However, before this distribution they go through a first metabolism in the liver. Some studies indicate that approximately 30% of the lost substances are reabsorbed by the intestinal tract through the bile.
Once reabsorbed, tricyclic antidepressants cross the blood-brain barrier. In fact, these antidepressants have a strong affinity for the brain and myocardium. Tricyclic antidepressants have 40 times more affinity with the brain and 5 times more with the myocardium compared to other tissues of the body.
Finally, they are metabolized in the liver and pass into the renal system for excretion. Most of the substance will be expelled within a maximum of 36 hours under normal conditions. This renal elimination is important to take into account in cases of overdose.
They take approximately two to four weeks to take effect. For real lasting changes to occur in the nervous system, they need to be taken for at least six months. Although in cases of recurrent depression, a longer treatment (two years or more) may be recommended.
After this cycle, the dose is gradually reduced until it is completely withdrawn. If it is stopped early, symptoms can return quickly. Also, if the dose is stopped abruptly, withdrawal symptoms may occur..
This entire process must be properly supervised by a qualified health professional.
Not all tricyclic antidepressants work in exactly the same way. Each one has small variations, allowing it to be adapted to the individual situation of each patient..
Generally, there are two classes of tricyclic antidepressants:
They have a greater effect on increasing serotonin than on norepinephrine. However, they cause greater sedation, greater anticholinergic effects (constipation, blurred vision, dry mouth) and hypotension..
Within this group, there are antidepressants such as imipramine (the first to be marketed), amitriptyline, trimipramine and doxepin.
Doxepin and amitriptyline appear to be the most sedating types of tricyclic antidepressants. Also, along with imipramine, they are the most likely to cause weight gain.
Tertiary amines are more suitable for depressed people with sleep problems, restlessness, and agitation.
They are those that increase the levels of norepinephrine more than those of serotonin, and cause irritability, over-stimulation and sleep disorders. They are recommended for depressed patients who feel dull, listless, and fatigued. An example of this type of tricyclic antidepressant is desipramine.
Some tricyclic antidepressants that should be mentioned are:
- Maprotiline: belongs to the group of secondary amines, and causes an increase in seizures.
- Amoxapine: it works as a serotonin receptor antagonist (which increases the amount of serotonin in the synapse). It has neuroleptic properties, so it can be recommended for those patients who have psychotic symptoms or manic episodes..
- Clomipramine: It is one of the most potent tricyclic antidepressants in terms of blocking the reuptake of serotonin, as well as norepinephrine. It has been shown to be effective in obsessive-compulsive disorder, although at high doses it increases the risk of seizures.
- Nortriptyline: like desipramine, it appears to be one of the tricyclic antidepressants with side effects that are better tolerated by patients.
- Protriptyline
- Lofepramine
One of the side effects of tricyclic antidepressants is the blocking of so-called alpha 1 adrenergic receptors. Causing a decrease in blood pressure, dizziness and drowsiness..
Tricyclic antidepressants, on the other hand, block acetylcholine (M1) receptors. This results in side effects such as blurred vision, constipation, dry mouth, and drowsiness..
Another effect produced by tricyclic antidepressants is the blockage of histamine H1 receptors in the brain. This results in an antihistamine effect, that is, drowsiness and weight gain (due to increased appetite).
Other associated side effects that have been observed are urinary retention, sedation, excessive sweating, tremors, sexual dysfunctions, confusion (mainly in the elderly), and overdose toxicity..
As tricyclic antidepressants cause sedation symptoms, driving or operating machines is not recommended. Since, if you are under its influence, the risk of suffering or causing accidents increases.
To reduce these problems and avoid daytime sleepiness, your doctor may advise that these drugs be taken at night; before sleep.
Suicidal wishes have been found in some adolescents and young adults after starting to take tricyclic antidepressants. Apparently, it is something that is linked to the first weeks of starting the medication or after increasing the dose.
Researchers do not know exactly if these ideas are due to depression itself or the effect of antidepressants.
Some believe it may be because the restlessness and agitation are more pronounced early in treatment. This can cause that, if there are some previous ideas of suicide (very common in depression), the depressed person feels with enough energy to commit it.
This risk appears to decrease as treatment progresses. However, if a sudden change is noticed, it is best to go to the professional as soon as possible..
Cases of abuse of tricyclic antidepressants or their misuse have been documented. For example, in healthy people with the goal of feeling more sociable and euphoric, followed by symptoms such as confusion, hallucinations, and temporary disorientation.
Tricyclic antidepressant poisoning is not uncommon. The lethal dose of desipramine, imipramine or amitriptyline is 15 mg per kg of body weight. Be careful with young children, as they could exceed this threshold with just one or two pills..
The abuse of this type of antidepressant can cause, in addition to the enhancement of the aforementioned secondary symptoms: tachycardia, fever, altered mental state, intestinal obstruction, stiffness, dry skin, dilated pupils, chest pain, respiratory depression, coma, and even death.
Sometimes tricyclic antidepressants can cause this syndrome, due to the excessive accumulation of serotonin in the nervous system.
However, most of the time it appears when antidepressants are combined with other substances that further increase serotonin levels. For example, other antidepressants, some drugs, pain relievers, or nutritional supplements like St. John's wort.
Signs and symptoms of this syndrome include: anxiety, agitation, sweating, confusion, tremors, fever, loss of coordination, and rapid heartbeat.
Tricyclic antidepressants are not considered addictive since they do not produce "craving" or desire to take them again. However, stopping them suddenly can cause withdrawal symptoms in some people. These can vary depending on the type of drug and do not last more than two weeks:
- Anxiety, restlessness, and agitation.
- Mood swings and low mood.
- Sleep disturbance.
- Tingling sensation.
- Dizziness and nausea.
- Flu-like symptoms.
- Diarrhea and stomach aches.
If antidepressants are gradually reduced to stop, these symptoms do not occur.
Yet No Comments