
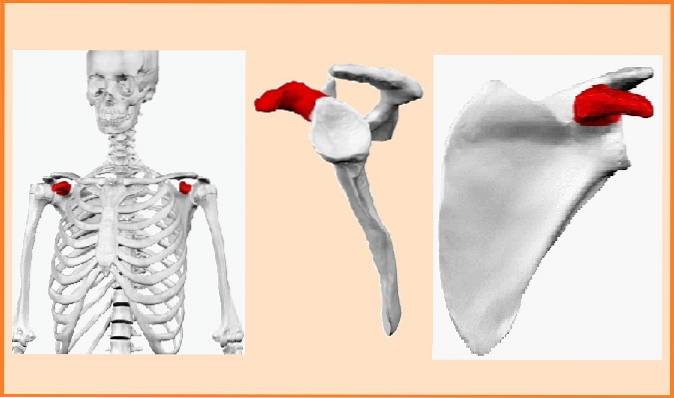
The coracoid process It is a bony protrusion that protrudes in the shape of a hook located on the shoulder blade or scapula, specifically on the anterior face and upper edge. Its base is wide and is in an upright position. In turn, the tip is finer and is arranged horizontally.
Sometimes it is called the coracoid process, derived from its Latin name processus coracoideus. This structure is located intermediate the glenoid cavity and the notch of the scapula..
It is a site of support and insertion of important muscles and ligaments of the shoulder. It is an even bone structure, that is, there is one on each side of the body. Among the muscles that have the coracoid process as an insertion point are: the pectoralis minor muscle, the coracobrachialis muscle and the short head muscle of the biceps brachii..
Among the ligaments that insert into the coracoid process are: the coracoclavicular ligament, made up of the Conoid Ligament and the Trapezoid Ligament. In addition, the coracoacromial and coracohumeral ligaments also join there.
The thoracoacromial artery that nourishes the acromioclavicular joint passes over the coracoid process.
The coracoid process can be palpated by placing the fingers below the clavicle, locating the infraclavicular fossa. From this point, the tip of the coracoid process can be palpated..
This structure is rarely affected by fracture, however, cases have been described in which it has fractured, due to traumatic accidents or by tearing of the ligaments that cause avulsion of the tip of the apophysis..
It has also been described as a cause of fracture of this bone structure, the traction of the acromioclavicular ligaments or the violent contracture of the muscles that are inserted in it..
Article index
The pectoralis minor, short head of the biceps, and the coracobrachialis are inserted at the level of the apex of the coracoid process. Whereas, the coracoclavicular ligaments and the coracoacromial ligament insert on the superior aspect and on the lateral border of the process, respectively..
The coracoid process is known for two very well defined functions: the first is the most obvious, it functions as an anchoring site for important muscles and ligaments found in the shoulder area. The second function it performs is the stabilization of the glenohumeral joint and the clavicle, due to the action exerted by the cone and trapezoid ligaments..
The low frequency reported in cases of fracture of the coracoid process is not accidental. This bone piece is anatomically protected by various structures.
In front it is protected by the rib cage and behind by a voluminous muscular environment. In addition, during trauma it is possible that the blow is cushioned thanks to the displacement of the scapula on the thorax.
However, fractures often occur in some car accidents or serious falls in athletes. When this occurs, the injury can occur at the level of three specific sites:
1) At the base.
2) Between the coracoclavicular and coracoacromial ligaments.
3) At the tip.
Injuries to the base are generally traumatic in origin, while the toe can occur due to tearing of the ligaments which, in turn, can detach part of the bone (avulsion).
It is a rare anomaly, first described in 1861. It consists of an unusual joint formed between the clavicle (cone tubercle) and the coracoid process (horizontal part). The joint has a diarthrosic synovial characteristic.
This anomaly has been more pronounced in Asian patients and generally presents bilaterally..
Delgado et al. In 2015, described a case in a 49-year-old woman who had pain in her shoulder and an X-ray revealed the congenital anomaly.
Acromioclavicular dislocation is a more or less frequent affectation that is generated by direct or indirect traumatic injuries of the shoulder, however in extremely rare cases the coracoid process suffers additional fracture. In this sense, three studies were reviewed.
Sánchez et al. In 1995 described a case of acrominoclavicular dislocation with a fracture of the base of the coracoid process. It was treated as follows:
The first 48 hours they placed an anti-edema bandage, called Robert Jones, then he was replaced by a shoulder orthosis. Is
used in 90 ° abduction for two weeks.
After two months, they performed an X-ray that showed consolidation of the coracoid process and a decrease in the acromioclavicular space below 5 mm. At 4 months there were no signs of pain and no limitation of movement of the shoulder. Therefore it was satisfactory.
On the other hand, González -Carranza et al. In 2001, reported a case of a 29-year-old woman who suffered an avulsion fracture of the coracoid process and dislocation of the acromioclavicular joint..
She was treated with oral analgesics and immobilization with a sling. At 4 weeks the bone callus was already visible radiographically and at 6 weeks it had fully formed. There was also a 90% recovery of shoulder mobility with very little pain.
Arbelo in 2003 described a case of fracture of the coracoid process in a 28-year-old young man. The case was associated with acromioclavicular dislocation and also presented with rupture of the coracoclavicular ligaments.
An open reduction technique and fixation of the coracoid process were performed, in addition to suturing the coracoclavicular ligaments. An excellent result was obtained.
Gutiérrez Blanco et al. Conducted a study to evaluate the efficacy of the dynamic stabilization of the acromioclavicular joint, through the transposition of the coracoid process to the lower edge of the clavicle..
They were later immobilized for two weeks using an inverted Vepeaux. Finally they applied a rehabilitation therapy. They obtained good results in most of the cases treated, with few exceptions.
This technique is recommended because it allows a 90% recovery of normal shoulder morphology, muscle strength, as well as shoulder mobility. However, some authors reject this technique because the appearance of long-term residual pain has been seen..



Yet No Comments