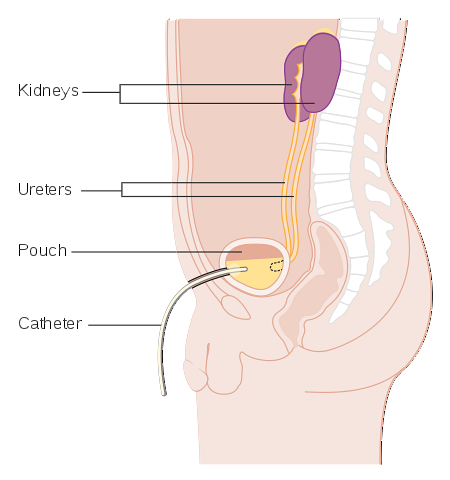
The cystostomy is a medical procedure that allows urine to be diverted from the bladder to the outside with the placement of a catheter through a suprapubic puncture or through a surgical incision of the bladder by the suprapubic route.
Cystostomy is indicated in obstructive pathologies of the urethra that prevent bladder emptying. It is indicated when the obstruction is complete and the bladder cannot be emptied using the urethral catheter..
There are records of the application of the cystostomy from Ancient Egypt and Ancient Greece, one of the first detailed references being attributed to Celsus, who describes the technique in order to perform a bladder lithotomy (extraction of "stones or stones").
The first to perform the suprapubic approach for bladder emptying was Pierre Franco in 1556. Then the surgeon Jean Baseilhac (1703-1781) developed an arrow-shaped guide that allowed the procedure to be carried out..
It is a common and widely used urological procedure with low morbidity. Various medical conditions require the use of a cystostomy and several techniques are available for the application of this procedure..
The cystostomy prevents urethral and penile injuries. It has a lower risk of infection than other techniques and reduces interference with the patient's sexual activity. It is a technique with high acceptance for patients in which it is applied.
Article index
The materials required for the procedure are the following:
-An antiseptic solution such as Povidone, Iodopovidone, Betadine, among others.
-gauze
-Gloves
-Fields
-Lidocaine 2%
-10 ml syringe
-Cistofix (R)
-Urine collector
-Thread (linen)
-Traumatic needle
-Dressings.
-First of all, the presence of complete urinary retention that requires emptying of the bladder must be confirmed as urine cannot be drained through the urethral catheter..
-Distended bladder confirmed by palpation.
-The patient is placed in a supine position (supine position).
-Gloves are put on.
-The suprapubic area is prepared. The suprapubic area is shaved and disinfected with the antiseptic solution.
-The fields are placed (sterile).
-We proceed to the placement of local anesthesia (2% lidocaine). It should be aspirated and applied progressively deepening and fan-shaped.
-The team is assembled (Cistofix).
-A puncture is made just above the pubis until reaching the bladder, at which time the urine begins to flow out, the probe is inserted about five centimeters more and the metal guide or mandrel is removed.
-The urine collector is connected and the catheter is fixed to the skin of the abdomen with a linen stitch.
-The fields are removed and the area is covered with a dressing.
Suprapubic cystostomy can be done by puncture or through a small surgical incision. In the first case, the catheter is inserted through a guide and then it is fixed to the skin. In the second case, the bladder wall is sutured to the skin.
Cystostomy may be temporary or temporary, while the obstruction resolves and bladder drainage through the urethra is restored; or it can be permanent when required.
There are several bladder catheterization techniques that try to minimize complications and develop increasingly safer methods. Open cystostomy is one of the first methods developed and still considered by many urologists as the safest method..
Open cystostomy requires a surgical intervention that aims to open a stoma (opening) in the bladder and abdomen, a stoma that will then allow the placement of the drainage cannula. This technique avoids visceral injuries during the procedure.
Currently, the cutaneous approach guided by an imaging procedure (fluoroscopy, ultrasonography) is increasingly used. These procedures are safe and reduce the risks of complications.
Direct percutaneous puncture techniques are often used in emergencies with large bladder distensions, in order to immediately empty the bladder and provide relief to the patient.
-You should wash your hands with soap and water whenever you need to handle the tube..
-You must ensure that the catheter drainage tube does not kink or “kink” and that -urine flows permanently into the collection bag..
-The urine collection bag should be kept below the level of the bladder.
-The urine collection bag should be held so that the catheter is not pulled or dragged.
-The patient can shower with the catheter and urine collection bag on, unless the doctor's prescription does not allow it.
-The collection bag should be emptied daily at least every eight hours or when full.
-Wash your hands with soap and water. If a patient's collection bag is being emptied and not your own, disposable gloves should be used.
-Remove the spout from the drain at the bottom of the collection bag and open the spout valve.
-Empty the urine from the bag into a container or down the toilet. The drainage tube or spout should not touch the container where the urine is emptied.
-Wipe up the liquid residue at the end of the drain opening with a gauze pad. Close the valve and close the drain again.
-Wash your hands again with soap and water.
-Acute retention of urine for different causes; in cases where the catheter cannot be inserted through the urethra.
-Some patients with neurogenic bladder.
-Persistent incontinence.
-Reflux vesicoureteral.
-Urethral injury. It can be temporary, while the urethra is rebuilding, or permanent, with irreparable urethral injuries.
-As a urinary diversion in patients with severe and disabling central neurological injuries.
-Patients with very prolonged urethral catheterization
-Patients with traumatic bladder injuries and urethral trauma that warrant temporary or permanent urinary diversion.
-Traumatic bladder injuries
-In patients with serious infectious processes in which the administration of high doses of antibiotics is required, cystostomy is used as a complementary management, in order to avoid bacteremia produced by urethral manipulation.



Yet No Comments