The dysglossia is a disorder of the articulation of the phonemes due to malformations or anatomical and / or physiological alterations of the peripheral articulatory organs. All of this hinders the linguistic functioning of people without detectable neurological or sensory impairments..
The causes that can originate dysglossia are congenital craniofacial malformations, growth disorders, peripheral paralysis and / or abnormalities acquired as a result of lesions in the orofacial structure or removals.
There are three aspects that can be related to dysglossia: intellectual deficiency to a variable degree, psychosocial deprivation and hearing loss. However, we must bear in mind that these aspects do not constitute a direct cause of dysglossia, although they do worsen the condition, since they make it difficult for the affected person to start compensatory mechanisms to improve spontaneous speech.
Article index
1 Symptoms
1.1 Nuclear symptomatology
1.2 Associated symptoms
2 Classification of dysglossia
2.1 -Labial dysglossia
2.2 -Mandibular dysglossia
2.3 -Dental disaggregates
2.4 -Lingual dysglossia
2.5 -Palatine dysglossia
3 Evaluation
3.1 Lips
3.2 Language
3.3 Hard palate
3.4 Soft palate
3.5 Breathing
3.6 Swallowing
3.7 Chewing
3.8 Phonation
3.9 Auditory discrimination of sounds
3.10 Auditory word discrimination
4 Treatments
5 References
Symptoms
Among the symptoms of dysglossia, we can distinguish, on the one hand, the nuclear symptoms, and on the other hand, the associated symptoms.
Nuclear symptomatology
The central symptomatology is characterized by an alteration in the articulation of different phonemes due to anatomical malformations of the peripheral organs of speech and of central non-neurological origin.
Associated symptoms
The symptoms associated with dysglossia are the presence of rhinophonias, which are voice alterations derived from lesions in the resonance cavities.
We find psychological disorders resulting from the speech problem, such as, for example, that the person with this disorder has a refusal to speak.
In addition, this disorder can be associated with school delay, difficulties in reading and writing, difficulties in normal fluency of speech, hearing loss (especially in cleft palate) and other difficulties that are related to long stays in hospitals.
On the other hand, we also find the lack of adequate stimulation for their level of development and the erroneous belief that dysglossia is inevitably associated with intellectual retardation..
Classification of dysglossia
-Lip dysglossia
Labial dysglossias are a disorder of the articulation of the phonemes due to the alteration of the shape, mobility, strength or consistency of the lips. Those that occur most frequently are due to:
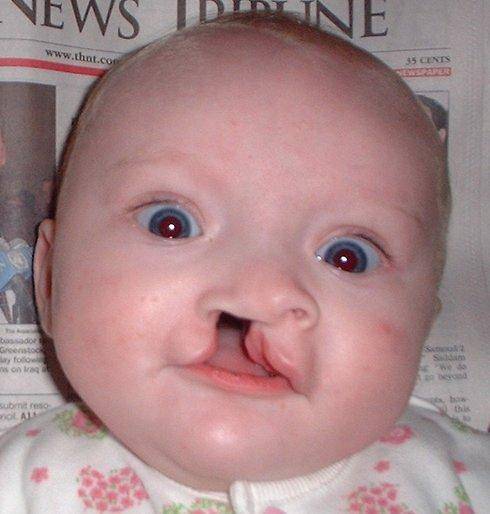
Harelip: it is a congenital anomaly that goes from the simple depression of the lip to its total cleft. The malformation can be unilateral and bilateral depending on the affected side. So the cleft lip can be unilateral or bilateral and simple or total. The most serious form of this malformation is called the middle or central cleft lip..
Hypertrophic upper lip frenulum: The membrane between the upper lip and the incisors develops excessively. They have difficulty articulating the phonemes / p, / b /, / m /, / u /.
Lower lip cleft: cleft in the lower lip.
Facial paralysis: frequently a consequence of forceps producing lesions and abnormalities in the middle ear. Have difficulty pronouncing the phonemes / f /, / n /, / o /, / u /.
Macrostomia: elongation of the oral cleft that can be associated with malformations in the ear.
Labial wounds: some wounds in the lip area that could cause alterations in the articulation of the phonemes.
Trigeminal neuralgia: sudden and short-lasting pain that appears on the face in the ophthalmic areas, upper and lower jaw.
-Mandibular dysglossia
Mandibular dysglossias refer to the alteration of the articulation of the phonemes produced by an alteration in the shape of one or both jaws.
The most frequent causes are:
Resection of jaws: the upper jaw is separated from the lower.
Mandibular atresia: anomaly caused by an arrest in the development of the lower jaw of congenital origin (endocrine disorders, rickets, etc.) or acquired (use of the pacifier, sucking the finger, etc.), which ends up producing a poor occlusion of the jaws.
Maxillofacial dysostosis: it is a rare hereditary disease that is characterized by a mandibular malformation derived from other anomalies and which gives rise to the typical “fish face” appearance.
Progeny: growth of the lower jaw causing mala occlusion of the jaws.
-Dental disglosses
Alteration of the shape and position of the teeth due to heredity, hormonal imbalances, diet, orthodontics or prosthetics.
-Lingual dysglossia
It is characterized by the alteration of the articulation of phonemes by an organic disorder of the tongue that affects the speed, accuracy and synchronization of the movements of the tongue.
The most frequent causes are:
Ankyloglossia or short frenulum: the membrane under the tongue is shorter than normal.
Glossectomy: total or partial removal of the tongue.
Macroglossia: excessive size of the tongue that causes breathing problems (characteristic of Down syndrome).
Congenital malformations of the tongue: arrest in embryological development.
Microglossia: minimum size of the tongue.
Hypoglossal palsy: when the tongue cannot move and there are problems speaking and chewing. It can be bilateral or unilateral.
-Palatal dysglossia
It is an alteration in the articulation of phonemes caused by organic alterations of the bone palate and the soft palate. Pathologies in which the normal structure is affected are called:
Palatal cleft: congenital malformation of the two halves of the palate seriously impeding swallowing and speech. Lip or palatal fissures originate in the first weeks of gestation.
Submucosal fissure: malformation where the palate is cleft.
Evaluation
To begin with the evaluation of dysglossia, it is appropriate to take an anamnesis to be able to know:
The reason for the evaluation.
Family background.
Pregnancy and childbirth.
Psychomotor development.
The development of speech.
The development of the dentition.
feeding.
Breathing (day and night -presence or not of snoring-).
Adenoid problems, tonsils, rhinitis and otitis.
Use of pacifiers, drooling, lip, finger, cheek, tongue, object sucking, object biting, etc..
Hospitalizations, surgical interventions and relevant diseases.
Medication.
Subsequently, we will proceed to the exhaustive evaluation of the oral organs:
Lips
Observe the lips at rest: we must indicate if they are closed, ajar or wide open.
Also, we must attend to the form of the same to know if they are symmetrical or asymmetrical, the shape of the upper and lower lip indicating if it is short, normal or long, and the presence of scars, as well as their location and characteristics.
The labial mobility It is evaluated by asking the child to move his lips to the sides, project them, stretch them, make them vibrate and wrinkle them as if to give a kiss. We will register if the lips move normally, with difficulty or there is no movement.
Tonicity: we will observe the lip tone through the kissing exercise and we will touch the upper and lower lip with our finger to notice their resistance and we will label it normotonia, hypertonia or hypotonia.
Lip frenulum: through observation we will evaluate if the upper or lower lip frenulum is short and if the upper one is hypertrophic.
Language
We will observe the tongue at rest and we will see if it is placed on the hard palate, interposed between the dental arches, pressing the arches laterally or projected on the upper or lower arch.
Shape: We ask the child to stick out his tongue and pay attention to the shape of the tongue, it can be normal, microglossia / macroglossia, wide / narrow and voluminous. It is important that we look for lateral marks of the teeth.
Mobility: the child is asked to move the tongue to the sides, raise it, project it, make it vibrate, etc. This way we will evaluate if it moves normally, with difficulty or there is no movement.
Tonicity: to detect the tone of the tongue we use a tongue depressor and push the tip of the tongue while the child resists. Through this exploration we can detect if the tongue is normotonic, hypertonic or hypotonic.
Frenulum: We ask the child to raise his tongue to verify his form. If we find it difficult, we ask you to suck your tongue against the hard palate and hold it. This allows us to see if the lingual frenulum is normal, short or with little elasticity.
Hard palate
Shape: when observing the palate we must look at the shape it presents, it can be normal, tall, pointed, wide or narrow, flat, short, with scars.
Palatal folds: observe if the folds of the hard palate are normal or hypertrophic.
Soft palate
We observe the soft palate at the end of the oral cavity. One of the elements that we must attend to is the uvula. When observing it, we must indicate if it has a bifid structure or if it is long, short or non-existent.
We must detect the presence of scars or fistulas in the white palate.
We will observe its dimension, indicating if it has a conventional dimension or is shorter than would be expected.
Mobility: to be able to observe the mobility of this area of the orophone we must ask the individual to emit the phoneme / a / during the examination. Thus we can see if mobility is good or is decreased or absent..
Dental / maxillary arches: see if the dentition is temporary, mixed or permanent.
Attend to the absence of teeth.
See if there is separation in the teeth, where and in what way can it influence language.
Malformation of teeth.
Indicate if you have dental prostheses, fixed or removable.
Gum condition: normal, swollen, or bleeding.
How is the person's bite.
Ability to open the mouth: difficult, does not open, dislodges the jaw, etc..
Observe if there is frontal symmetry between the right and left sides of the face.
Facial profile: normal, retrusion, or forward projection of the mandible.
Another relevant aspect for dysglossia is the evaluation of orofacial functions. To do this, we must attend:
Breathing
Observe if breathing occurs in a nasal, oral or mixed manner, if there is respiratory coordination. In addition, it is also important to assess murmur control and measure lung capacity..
Swallowing
To evaluate the way of swallowing, the individual is offered water or yogurt and we observe the placement of the lips, the leg and the pressure that is exerted to be able to swallow the food.
Chewing
To evaluate chewing, the subject is offered a food such as donuts or cookies and the movements carried out with the mouth and with the tongue are evaluated..
Phonation
It is important to pay attention to the tone of voice, the existence or not of hypernasality and the existence of articulatory difficulties.
Auditory discrimination of sounds
Sounds of everyday objects are introduced and you are asked to identify them. For example, sounds of coins or paper crumpling.
Auditory word discrimination
Words with similar phonemes are presented and the person has to identify the difference.
Treatments
In the treatment of dysglossia, it is important that a multidisciplinary intervention is carried out given the nature and character of this language disorder..
Because dysgloisa is a disorder that affects various areas of the individual, through the coordination of a team of professionals we can ensure that the patient can achieve normative development. The professionals that would make up this multidisciplinary team would be:
Neonatologist: is the first professional with whom the child comes into contact and with whom the treatment begins. This professional performs rapid evaluations of neonatal growth and development, is that he performs an evaluation of the anomaly or malformation detected and thus will be able to determine the best way of feeding and will mobilize the available resources so that the child is intervened by the team.
Pediatrician: he is the one who will carry out the follow-up, he is the professional who has direct contact with the parents and has the mission of informing and accompanying during the treatment. In addition, they must be in communication with the other members of the multidisciplinary team.
Orthodontist: it is the professional who is in charge of correcting initially and during the evolution of the treatment a correct dentition, accommodation of the palate and teeth.
Speech therapist: specialist who will treat the functional part of the initial part of the digestive and respiratory system. The objective is for the individual to achieve a correct phonation function.
Psychologist: This professional will work with the parents and the child. On the one hand, in the first place the work will be directed towards the parents to try to alleviate the pain they feel in the face of the malformation and the treatment of their child. On the other hand, the psychologist will work directly with the child so that he can achieve a normalized social integration and that he has adequate self-esteem.
Surgeon: coordinates the treatment by explaining, supporting and sending the child to consult and join the treatment until the surgical correction is made. It is convenient to start surgical treatment during childhood so that the orophonatory organs that are altered can be repaired before speech begins. Operations are likely to be repeated when the patient is an adult.
Othersprofessionals: social workers, cosmetic surgeons, otolaryngologists, anesthetists, etc..
References
Belloch, A., Sandín, B., and Ramos, F. (2011). Manual of psychopathology (vol. 1 and 2) McGraw-Hill: Madrid.
Díaz, A. (2011). Difficulties in language acquisition. Innovation and educational experiences 39.
Soto, M.P. (2009). Language assessment in a student with dysglossia. Innovation and educational experiences 15.
Prieto, M. A. (2010). Alterations in language acquisition. Innovation and educational experiences 36.
De los Santos, M. (2009). The dysglossia. Innovation and educational experiences 15.



Yet No Comments