
Entamoeba gingivalis it is a commensal protozoan of the oral cavity that lives in gums, dental tartar and tonsillar crypts. Some authors claim that it has been found outside the mouth, especially in smears from the vagina and cervix of women with devices. It has also been seen in captive primates, horses, dogs and cats..
This microorganism was discovered by G. Gros in 1849. At that time it was called Endamoeba gingivalis and it was considered a commensal microorganism. Although this finding was observed in some patients suffering from periodontitis, there was no association of this pathology with the presence of the amoeba, a situation that lasted for more than a century.
In 1980 T. Lyons rescued interest in the Entamoeba gingivalis, after he detected amoeboid microorganisms in periodontal pockets, and observed that these were absent in healthy sites.
Lyons suspected that the pathology could be related to the amoeba, so he implemented a treatment based on oxygen peroxide and metronidazole, with which he was successful..
However, that was not enough to classify E. gingivalis as a causal agent of periodontitis. There have been many studies on this in particular and there are still controversies about it.
Article index
Entamoeba gingivalis it is a non-invasive microorganism, as it does not spread outside its usual ecological niche.
There is a prevalence ranging from 6% to 80% of E. gingivalis in patients with oral affectations such as gingivitis, advanced periodontal disease, dental caries, abscesses or oral suppurations, dental prostheses and in biofilms formed at the base of the teeth.
However, it has also been found in patients with good oral health, but less frequently. Therefore, it has not been possible to define it as a pathogen, but perhaps it behaves more like an opportunist.
The normal microbiotas in living organisms are generally maintained without causing discomfort to the host as long as they are in perfect balance, but if for some reason one microorganism is exacerbated over others, there may be consequences..
Therefore, if the parasite proliferates more than normal, it could create an imbalance in the oral microbiota. That is how Entamoeba gingivalis can generate an inflammatory, degenerative and necrotic response in the gums and surrounding connective tissues, which promote microbial colonization in the periodontal pockets.
Although it is not the causal agent of the disease, it can contribute to its occurrence, acting together with the bacteria. On the other hand, it has been speculated that the presence of some bacteria in the oral microbiota is favorable for reducing oral pathologies. For example, Porphyromonas catoniae Y Neisseria flavescens.
Therefore, they are considered passive indicators of oral health, but it is unknown if their presence limits to E. gingivalis. What is known is that Entamoebas gingivalis feeds on flaking cells at the gum line, blood cells, and bacteria.
They also phagocytose the nuclei of polymorphonuclear cells, through a mechanism called exonucleophagy..
Entamoeba gingivalis belongs to Kingdom Protista, Phylum: Amoebozoa, Class: Archamoebae, Order: Mastigamoebida, Family: Entamoebidae, Genus: Entamoeba, Species: gingivalis.
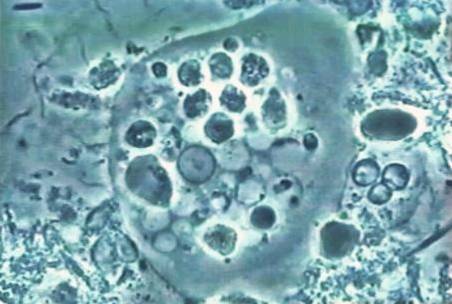
The trophozoite is unicellular in which a clear external ectoplasm and an internal granular endoplasm are distinguished. Only the vegetative or trophozoite form is known, measuring 5-35 µm..
Entamoeba gingivalis it has a non-mobile stage, where the ectoplasm is barely visible, and a mobile phase where it appears as a thick layer that comprises approximately half the volume of the trophozoite.
It has a small central vesicular nucleus of 2 to 4 µm with a thin nuclear membrane, lined with fine chromatin granules grouped in the periphery. They contain a central or eccentric karyosome.
The endoplasm is granular and vacuolated. It is normally full of floating food particles.
Food vacuoles contain dark rounded bodies, derived largely from the nuclei of degenerated epithelial cells, lymphocytes, and occasionally leukocytes.. E. gingivalis also ingest bacteria but to a lesser extent.
Basically E. gingivalis is a disintegrated cell remover.
The cytoplasm is finely granular and presents multidirectional ectoplasmic pseudopods that allow it to move.
It is unknown if it has the ability to encyst as other amoebas do..
Entamoebas can be observed under the light microscope of samples taken from the ecological niches of the parasite. For this, smears stained with special stains such as gomori methenamine silver (GMS), periodic acid - Schiff (PAS), iron hematoxylin, giemsa and papanicolaou can be made..
However, some authors state that these stains do not allow the structures of the microorganism to be well visualized, making it difficult to observe the nucleus because the vacuoles overlap.
Therefore, highly skilled professionals are needed for the identification of amoeba, since it is easily confused with histiocytes. For this reason, they recommend making fresh preparations, making mouthwashes with 3 mL of saline solution..
Subsequently, the sample is centrifuged and a drop of sediment is dispensed onto a slide, covering it with a cover sheet..
In this simple preparation, all the structures of the parasite can be visualized in vivo, where the characteristic movement of the trophozoites can even be appreciated..
It can be transmitted through intimate contact with the saliva of people who present Entamoeba gingivalis in his mouth.
This means that the Entamoeba gingivalis It is transmitted by deep kissing, drinking or eating with glasses and cutlery contaminated with saliva from people that contain the protozoan in their oral cavity. Also because of the shared use of toothbrushes.
Risk factors for presenting the parasite with active symptoms in the oral cavity include:
All of them are believed to play a key role in the proliferation of the microorganism..
The Entamoeba gingivalis it reproduces by longitudinal binary division and does not present sexual reproduction. The cycle begins when a susceptible person is exposed to saliva contaminated with the parasite, either direct or indirect..
Once the Entamoeba reaches the new host, the trophozoite begins its division. If it achieves favorable conditions, it is installed in various ecological niches, where it remains.
They can disappear if good oral hygiene is maintained.
Oral hygiene and good dental control is recommended to maintain good oral health.
You should go to the dentist when certain manifestations occur such as: halitosis, very red gums, frequent bleeding and itching in the gingival area.
In this way, these discomforts will be prevented from progressing to severe periodontal diseases..
Non-surgical periodontal treatment could reduce the number of Entamoeba gingivalis in the oral environment of patients with chronic periodontitis.
An in vitro study showed that metronidazole eliminates E. gingivalis at a concentration ≥ 4 mg / L.
Likewise, an in vivo clinical study reported a 64% to 26% decrease in E. gingivalis in periodontal disease, after treatment with oral metronidazole, 750 mg daily for 7 days.


Yet No Comments