
The pathophysiology of depression it is based on differences in brain structures such as the size of the amygdala, hippocampus or prefrontal cortex. Likewise, changes have been found in neuronal size, glial density and metabolism. The role of monoamines or other neurotransmitters has also been documented and various theories have also been offered about their genesis or explanation..
Depression is not exclusively due to biological or psychological factors, but rather is due to the complex interaction of numerous social, psychological or biological factors.

When looking for the best treatment to deal with depression, and taking into account that pharmacotherapy (and the different antidepressants) have also reacted unfavorably in many aspects, we have sought what are the processes that are involved in this disease.
Article index
The tendency to develop a depressive disorder seems to be due, in some way, to heredity. This information comes to us through family studies, so that a person with a close relative with an affective disorder is 10 more likely to suffer from it than another person who does not have an affected relative.
These data indicate that depressive disorders have a hereditary tendency. In addition, this can also be observed through studies of monozygotic twins, which show that there is a greater concordance between these in depression than in dizygotic twins.
Along the same lines, adoption and depression studies indicate that there is a higher incidence of depression in biological parents than in adoptive parents.
In relation to the genes involved in depression, research indicates that there are multiple genes involved, observing linkage between genes that are located on chromosomes 2, 10, 11, 17, 18, among others, as well as polymorphisms of genes such as that of the serotonin transporter in terms of the origin of depression.
Obviously, if we are referring to a disease with multiple symptoms and where the variability is great, it is logical to think that the genes involved are multiple as well..
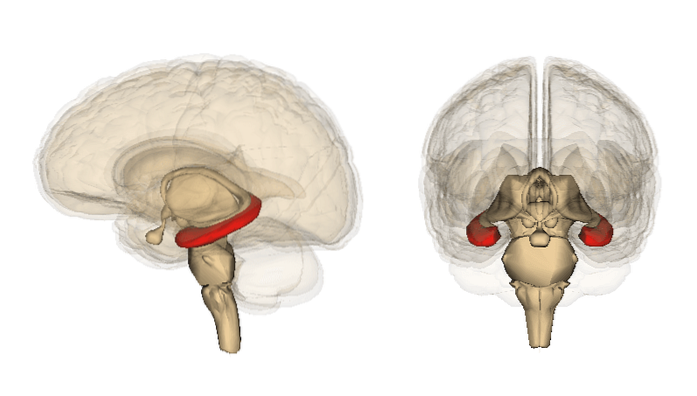
Several neuroimaging studies have been carried out with depressive patients that have shown that they present alterations in different brain structures. Among them, we highlight the alterations in the amygdala, in the hippocampus and in the prefrontal cortex, both dorso-lateral and ventral.
Regarding the hippocampus, some studies have found decreased white matter and have shown that there is an asymmetry between the hemispheres, as well as less volume in both hippocampus in patients with depression.
At the anatomical level, in general, gray matter has been found to be reduced in the orbital and middle prefrontal cortex areas, in the ventral striatum, in the hippocampus and an elongation of the lateral and third ventricles, which implies a neuronal loss.
In other studies, once the patients were already dead, a decreased volume of the cortex and glial cells has been found.
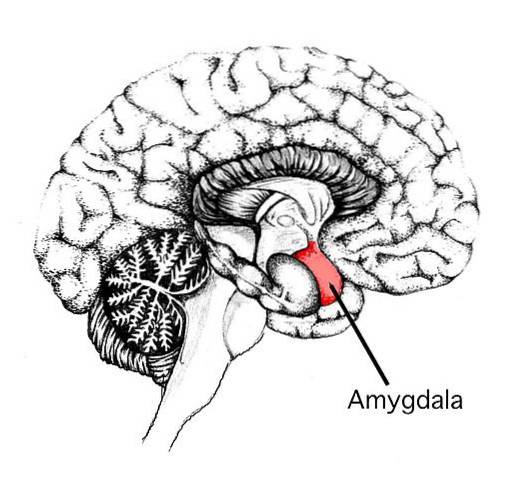
In relation to the amygdala, the studies show variable results. Although there have been no differences in terms of the volume of the amygdala, some of its characteristics did..
For example, the medication explained differences in the volume of the amygdala, so that the more people with medication there were in the study, the greater the volume of the amygdala of the patients with depression compared to the control.
These types of results could contribute and reinforce the idea that depression is associated with a decrease in the volume of the amygdala.
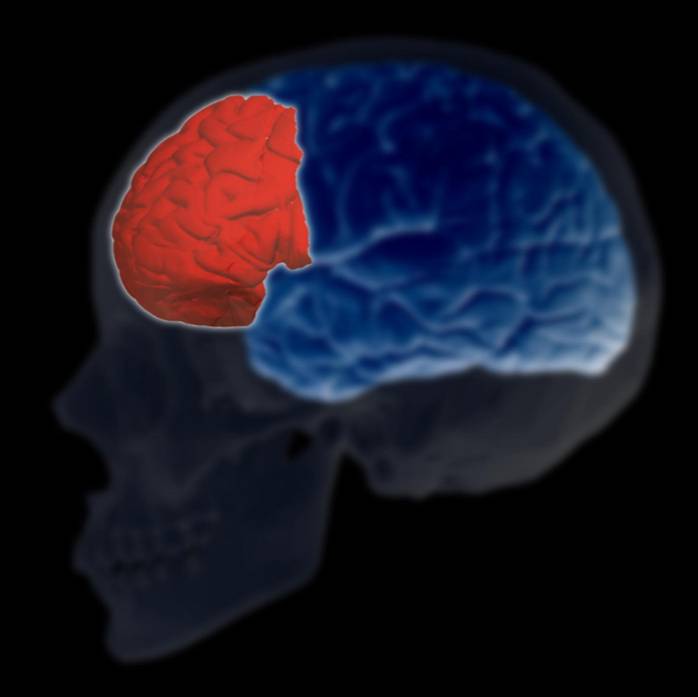
Regarding the prefrontal cortex, various studies have also found that patients with depression had less volume compared to the control in the rectus gyrus and not in other different regions.
Regarding brain activity, neuroimaging studies have also shown abnormalities found in blood flow and glucose metabolism in depressed subjects.
Thus, it has been suggested that increased metabolism in the amygdala was related to a greater severity of depression, while when metabolic activity in the ventromedial prefrontal cortex was reduced, they are too reactive to induced sadness but hyporeactive to depression. induced happiness.
In other studies, it was shown that there was a correlation between the severity of depression and increased glucose metabolism also in other regions such as the limbic system, ventromedial prefrontal cortex, temporal, thalamus, ventral areas of the basal ganglia or the inferior parietal cortex.
Loss of motivation in depression was also negatively related to certain areas, with the dorsolateral prefrontal cortex, the dorsal parietal cortex, or the dorsotemporal association cortex..
There was also a relationship in sleep, so that its alterations were correlated with greater activity in some cortical and subcortical areas.
There are some circuits that are related to depression, among which we can highlight, for example, the appetite and weight gain that occurs in some patients with depression.
Depressive mood, the main symptom of depression, is related to alterations that occur in the amygdala, in the ventromedial prefrontal cortex and in the anterior cingulate gyrus, involving both serotonin, dopamine and norepinephrine.
For its part, the lack of energy that also characterizes patients with depression is related to dopamine and norepinephrine and addresses the problems found in the diffuse prefrontal cortex.
Sleep disturbances are also related to dysfunctions of the hypothalamus, thalamus, basal forebrain and where norepinephrine, serotonin and dopamine are involved..
For its part, we found that apathy is related to a dysfunction of the dorsolaterl prefrontal cortex, the nucleus accumbens, and norepinephrine and dopamine are important neurotransmitters..
The psychomotor symptoms that we find in depression are associated with alterations of the striatum, cerebellum and prefrontal cortex, being associated with the three monoamines.
For their part, executive-type problems are related to dopamine and norepinephrine and are associated with the dorsolateral prefrontal cortex.
There are various theories or hypotheses that have been gathered around the origin of depression.
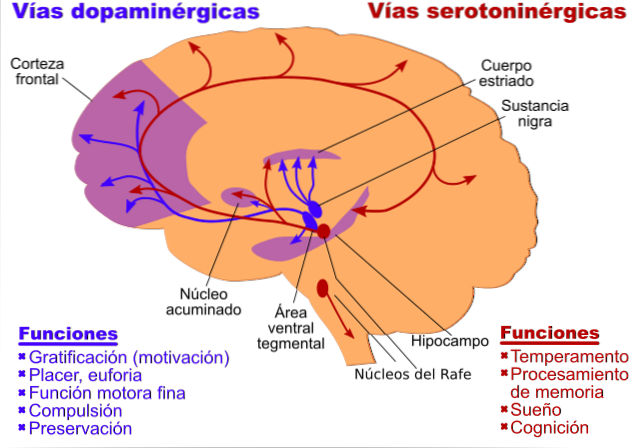
One of them, the first, arises around the idea or hypothesis that a deficit of monoamine neurotransmitters, such as norepinephrine, dopamine or serotonin, would be the cause of depression. This is the monoaminergic hypothesis of depression.
This hypothesis is based on different evidences. One of them, for example, is the fact that reserpine (a drug for hypertension) caused depression; it acts by inhibiting the storage of monoamines and acting antagonistically to monomines. Thus, it is suggested that it can lead to depression.
In the opposite case, we find the drugs that enhance these neurotransmitters and that improve the symptoms of depression, acting as agonists..
It should also be noted that there are data that did not support this hypothesis, the definitive proof against this hypothesis being the fact of what is called therapeutic latency, which explains the delayed improvement that occurs in the symptoms of depression after the administration of the drug. which indicates that there must be some intermediate process that takes care of said improvement.
It is proposed that there may be some other mechanism in the brain that does not correspond only to monoamines and that are responsible for depression.
A possible explanatory mechanism is the receptors, so that in depression there could be an alteration of them, an upregulation that is due to the fact that there is a deficit of the neurotransmitter. When not enough is produced, over time there is an increase in the number and sensitivity of the receptors.
Evidence of this hypothesis is also found, such as studies of suicidal people that postmortem allow finding this increase in receptors in the frontal cortex.
Other evidence would be the same fact that the antidepressants that are taken produce desensitization in the receptors.
More recent research suggests that it could be due to an abnormality in the gene expression of the receptors (due to deficit or malfunction).
Other lines suggest, rather, that it could be due to an emotional dysfunction of mechanisms such as alterations in the gene for the neurotrophic factor derived from the brain that supports the viability of neurons.



Yet No Comments