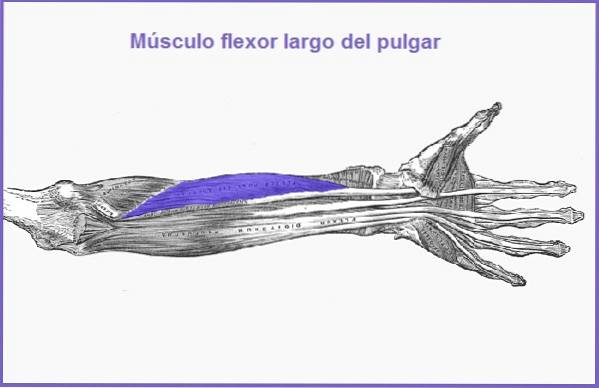
The long flexor of the thumb It is a muscle that has the purpose of causing the flexion of the thumb and indirectly contributes to the movement of the hand. It's even, flat, and, as the name suggests, long. Its name comes from the Latin musculus flexor pollicis longus.
The flexor pollicis longus muscle can be injured by trauma. The symptoms are mainly due to the injury or compression of the interosseous nerve that innervates this muscle.
This type of injury causes muscle weakness or difficulty grasping objects with the fingers. Especially the ability to bring the thumb and index finger together in a pincer shape is affected. There is also pain in the forearm.
Another important factor that has been related to compression of the interosseous nerve is the finding of unusual muscular anatomical variants at the level of the nerve trajectory. Such is the case of the presence of the accessory fascicle of the flexor longus muscle, which affects a small group of individuals..
Article index
It is a long, flat, even muscle. It is located laterally to the deep common flexor muscle of the fingers. It runs from the tuberosity of the radius, passes in front of the pronator quadratus muscle, until it reaches the thumb. The fibers of the flexor longus muscle are oriented obliquely.
The flexor pollicis longus muscle originates from the forearm in its proximal third, on the anterior aspect of the radius (tuberosity), and on the interosseous membrane.
The flexor pollicis longus muscle attaches at the base of the distal or nail phalanx of the thumb, on its anterior or palmar aspect..
The flexor longus muscle has the function of flexing the distal phalanx of the first finger (thumb). This folds over the proximal phalanx and the latter over the first metacarpal, that is, it moves the metacarpophalangeal joint, the proximal interphalangeal joint and the distal joint..
It also has an indirect or accessory function in the movement of the wrist..
This muscle is very useful in our daily life, since it allows us to make fine tweezers to hold small objects, such as holding a pencil, etc., as well as thick tweezers, that is, larger objects taken with the thumb and index finger. , being an example of this grab a glass.
This muscle is innervated by the anterior interosseous nerve, whose function is purely motor. This nerve comes from the trunk of the median nerve.
The flexor pollicis longus muscle is supplied by the anterior interosseous artery.
This pathology is characterized by the appearance of pain in the anterior aspect of the forearm, specifically at the level of the proximal third. The patient finds it difficult to grasp things using the fingers as forceps, as well as there may be difficulty in pronation.
All this is caused by compression of the interosseous nerve, affecting the mobility of the muscles it innervates, that is, the long flexor of the thumb, the deep flexor muscle of the index and middle and the pronator quadratus..
If the median nerve is affected in compression, the patient complains of pain radiating towards the wrist.
The origin of the compression can be due to forearm fractures, puncture wounds or caused by long-range firearms.
Treatment in most cases is non-invasive, that is, the arm is immobilized for 8 to 12 weeks and non-steroidal anti-inflammatory drugs are placed..
It should be noted that there is another cause that can compress the interosseous nerve, as some people may present an anatomical variant called the accessory bundle of the flexor longus muscle..
The presence of anatomical variants can lead to the formation of additional fibrous arches that compress the anterior interosseous nerve. This muscle variant can present unilaterally or bilaterally..
It was first described in 1978 by Lindburg. This syndrome is characterized by the inability of the patient to flex the interphalangeal joint of the thumb in isolation, since doing so also flexes the distal interphalangeal joint of the index finger.
Another finding that confirms the diagnosis is the appearance of pain when the patient flexes the thumb and the examiner tries to resist the action.
This syndrome is caused by the abnormal presence of anatomical communications, which interconnect the long flexor muscle of the thumb and the flexor muscle of the index finger. This abnormality can occur unilaterally or bilaterally..
This condition is usually associated with carpal tunnel syndrome. Treatment is almost always surgical.
The flexor tendons together cause the hand to assume a characteristic position when it is completely at rest. This position resembles a waterfall, hence this position is called "normal cascade of the fingers".
In this position, the thumb and index finger are slightly flexed. It increases as you advance to the next fingers, that is, the middle finger will be slightly more flexed than the index and the little finger more arched than the middle finger..

Knowledge of this physiological behavior is of utmost importance for hand surgeons, since when they perform surgery on an injured finger, it must take this form after the procedure has been performed..
If a flexor tendon is injured, its function, which is to tension to be able to bend the finger, is lost, therefore, the extensor tendon dominates, leaving the finger permanently extended. In this case, flexor muscle damage is evident and no exploratory procedure is necessary..
If the injury is partial and at the level of the deep flexors, the following examination maneuver is described:
The proximal interphalangeal joint of the injured finger should be immobilized and the patient is then instructed to try to flex the finger (distal phalanx). If you can do this, it means that the deep flexor muscles are working well..
For complete rehabilitation of the injured flexor muscle to be achieved, a correct surgical technique must be followed, plus an adequate number of therapeutic sessions with a professional trained in hand injuries..



Yet No Comments