The fluoxetine, better known as prozac,is an antidepressant that falls under the category of selective serotonin reuptake inhibitors (SSRIs). Better known as Prozac, it is one of the most widely prescribed antidepressants worldwide. Although it has numerous beneficial effects to treat disorders such as depression or anxiety, it cannot be taken lightly, as it can also cause adverse effects.
The appearance of the SSRIs in the late 1980s revolutionized psychopharmacology, reaching up to six prescriptions per second. Although they were originally born as antidepressants, they are also often prescribed for other less serious conditions such as premenstrual dysphoric disorder, anxiety disorders or some eating disorders.

Within the group of SSRIs there are six types of compounds that share many effects, although they also have unique properties that differentiate them. In this article we will see the common effects and those of flouxetine..
Article index
To understand fluoxetine, and the general SSRIs, it is necessary to know what happens in the brain of a person with depression at the cellular level.
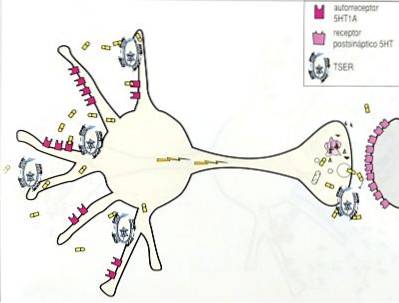
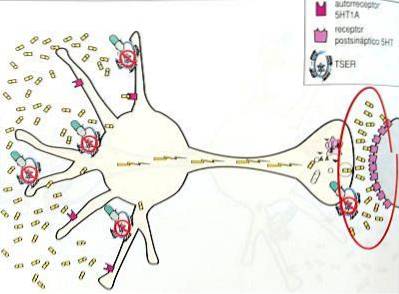
According to the monoaminergic hypothesis, people with depression suffer from a deficiency of serotonin in the presynaptic serotonergic neurons, both in the somatodendritic areas and in the axon terminal.
All antidepressants act by increasing serotonin to its previous levels, prior to the disorder, and in this way they try to alleviate or end depressive symptoms.
In addition to acting on axonal receptors, SSRIs act on serotonin receptors in the somatodendritic area (5HT1A receptors), and this triggers a series of effects that end with an increase in serotonin.
The mechanism of action of SSRIs will be explained step by step below:
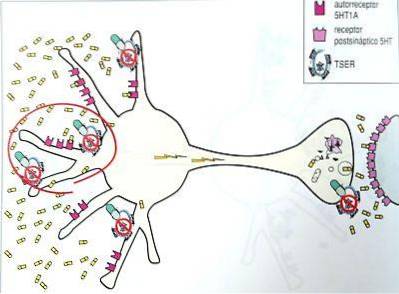
SSRIs block serotonin receptors in the somatodendritic area, also called TSER (serotonin transporter) pumps. This blockage prevents serotonin molecules from binding to receptors and therefore serotonin cannot be reuptained (hence the name SSRIs) and remains in the somatodendritic area..
After a while serotonin levels rise due to its accumulation. Serotonin levels also increase in unwanted areas and the first side effects begin to be observed.
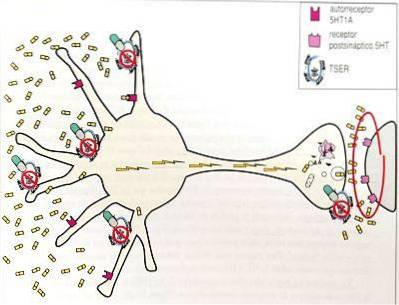
When the receptors have been blocked for a while, the neuron "identifies" them as unnecessary, for this reason they stop working and some disappear. These effects are known as desensitization and down regulation and occur through a genomic mechanism..
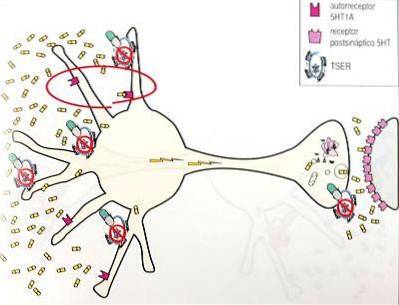
As there are fewer receptors, the amount of serotonin that reaches the neuron is less than before regulation. Therefore, the neuron "believes" that there is too little serotonin, begins to produce more amounts of this neurotransmitter and its flow to the axons and its release is activated. This mechanism is the one that explains most of the antidepressant effects of SSRIs..
Once the neuron has already begun to secrete higher levels of serotonin, another mechanism of action of SSRIs begins to be relevant that had not been effective so far.
This mechanism is the blocking of axonal receptors, which are also desensitized and down-regulated, and therefore less serotonin is reuptained. This mechanism causes the side effects of the SSRI to begin to lessen, since serotonin levels are lowered to normal levels..
In short, SSRIs act by progressively increasing serotonin levels in all brain areas where serotonergic neurons are present, not just where they are needed, which causes both beneficial and harmful effects. Although the unwanted or side effects get better over time.
In addition to the mechanism explained above, common to all SSRIs, fluoxetine also follows other mechanisms that make it unique.
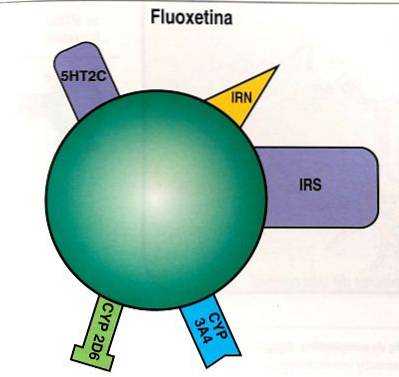
This drug not only inhibits the reuptake of serotonin, it also inhibits the reuptake of norepinephrine and dopamine in the prefrontal cortex, blocking the 5HT2C receptors, which increases the levels of these neurotransmitters in that area. The drugs that have this effect are called DIND (norepinephrine and dopamine disinhibitors), therefore, fluoxetine would be a DIND in addition to an SSRI.
This mechanism may explain some of the properties of fluoxetine as an activator, thus helping to reduce fatigue in patients with reduced positive affect, hypersomnia, psychomotor retardation and apathy. On the other hand, it is not advisable for patients with agitation, insomnia and anxiety, since they may experience unwanted activation.
The mechanism of fluoxetine as DIND may also act as a therapeutic effect on anorexia and bulimia.
Finally, this mechanism may also explain the ability of fluoxetine to increase the antidepressant actions of olanzapine in patients with bipolar depression, since this drug also acts as DIND and both actions would be added..
Other effects of fluoxetine are the weak blockade of norepinephrine reuptake (NRI) and, at high doses, the inhibition of CYP2D6 and 3 A4, which can increase the effect of other psychotropic drugs in an undesired way..
Furthermore, both fluoxetine and its metabolite have a long half-life (2 or 3 days for fluoxetine and 2 weeks for its metabolite), which helps reduce the withdrawal syndrome observed when withdrawing some SSRIs. But keep in mind that this also implies that it will take a long time for the drug to completely disappear from the body when the treatment ends..
Among the side effects shared by fluoxetine and in general all SSRIs are:
In addition to the effects just mentioned, fluoxetine can cause other side effects of its own that can be seen in the following table..
If an overdose of fluoxetine occurs, instability, confusion, lack of response to stimuli, dizziness, fainting and even coma may occur, in addition to the above side effects..
Furthermore, the pre-marketing clinical study of the drug found that some of the younger participants (under 24 years of age) developed suicidal tendencies (thought or tried to harm or commit suicide) after taking fluoxetine. Therefore, young people should be especially cautious with this drug..
psychotropic drugs can be very dangerous for health in general and especially for mental health; For this reason, they should never be self-administered, they must always be taken after the medical prescription and during their taking, you should see a doctor if you notice any mental or physical change.
It is important to inform your doctor if you are taking, or have just stopped taking, any other drug as it can interact with fluoxetine and cause harmful effects..
Below you will find a list of medications that can be potentially dangerous if combined with fluoxetine:
It is also advisable to notify your doctor if you are taking vitamins, such as tryptophan, or herbal products, such as St. John's wort..
In addition, special care must be taken with fluoxetine if you are receiving electroconvulsive therapy, if you have diabetes, seizures or liver disease, and if you have recently suffered a heart attack..
Fluoxetine should not be taken if you are pregnant, especially in the last months of pregnancy. It is also not recommended that people over 65 take this drug..



Yet No Comments