The phrenilectomy or frenectomy It is the intervention that consists of the section or cut of the frenulum. However, we must clarify that we find three braces in our body that may require surgery, and each of them will require the intervention of a different specialist.
Likewise, both the indications and the techniques to be used in each one are of course different as well. Let's review each of these braces and what is derived from each of them.
Article index
The upper lip frenulum is a band of fibrous, muscular tissue or both that usually joins the upper lip with the gum. In fact, there is an upper and a lower one. Its function is to keep the mucosa of the cheeks, tongue and lips fixed to the alveolar mucosa, gums and periosteum..
When its anatomy is preserved, its base occupies the upper two-thirds of the gingiva and continues its ascent until it joins and fuses with the upper lip. The problem arises when there is an abnormal development of any of the braces (generally the upper one), which will lead to dental and speech problems.

The fundamental indication for surgery of the upper labial frenulum is given when, due to its origin, very low insertion and thickness, it causes what is called the diastema (or separation) of the upper incisors, deforming the dental arch and causing an unsightly condition that requires its resolution..
A diastema will also cause problems of perfect dental occlusion. Another indication arises when the proximity of the insertion to the gingival margin produces a gingival resection or alters oral hygiene..
Additionally, the presence of this exaggerated frenulum will make it impossible to properly move the upper lip when speaking, limiting the pronunciation of some phonemes, with consequent speech problems..
In any of these cases, upper labial frenilectomy is indicated..
The lower lip frenulum very rarely causes any kind of problems, even when it is short and thick..
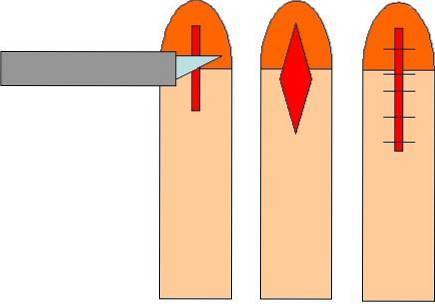
It can be performed using conventional techniques (classical, Miller, rhomboid, etc.) or laser techniques.
To perform conventional techniques, if the patient collaborates, the intervention can be performed in the office with infiltrative local anesthesia. The goal is complete removal, including its adherence to the bone.
It can be performed by the dentist duly trained in the procedure or the oral-maxillo-facial surgeon.
The anesthesia is infiltrated and it is waited for its effect to take place. At the moment of instilling it, adrenaline can be instilled together, which will cause vasoconstriction, thus reducing bleeding.
There are two possible interventions:
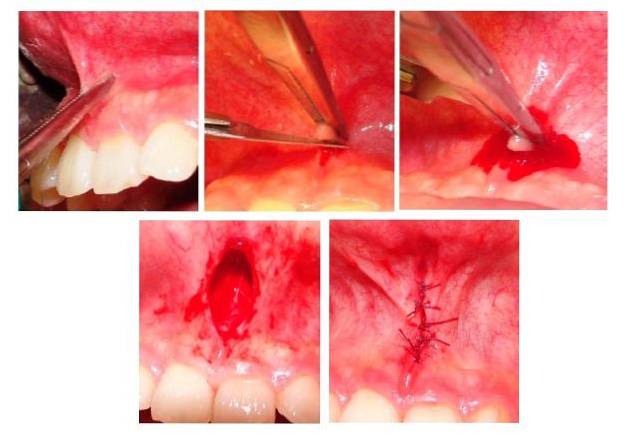
In both cases, once the cut has been made (which can be with a manual scalpel, or an electrosurgical knife), resorbable suture is placed in both the labial and gingival portions, to avoid subsequent bleeding..
It is complemented with the indication of analgesics-anti-inflammatory or physical means (cryotherapy) for at least 48 hours, or as required by the patient. Because the suture is resorbable, it does not need to be removed as it will fall off on its own.
The laser technique (CO2, Nd-YAG, Er-YAG or diode laser) removes the frenulum in a faster way and with many more advantages.
It does not need anesthesia, it causes less pain, better visibility when operating, better healing and less scarring, it allows to sterilize the area and does not require the use of sutures.
Normally, the lingual frenulum is a thin mucous membrane that joins the base of the tongue with the floor of the mouth. When it limits the movements of the tongue, and with them makes speech difficult, we are in the presence of a short lingual frenulum or ankyloglossia.
Ankyloglossia means "anchored tongue," and it is a congenital disorder that has varying degrees of severity. Four types of lingual braces are defined:

If the frenulum prevents the child from moistening the lower lip with his tongue normally, there is an indication for frenilectomy.
If you limit breastfeeding in young infants or limit language in older infants and preschoolers, there is also an indication for frenilectomy.
It can be performed by a pediatrician duly trained in the procedure, a pediatric surgeon, a pediatric dentist with training in the procedure, or an oral-maxillofacial surgeon..
Depending on the age of the child, it may be practiced in the office or it may be necessary to take the minor to the operating room, to guarantee their immobility during the procedure..
If it is an infant under 6 months, it can be done in the office with or without local anesthesia (younger, less need for anesthesia). A spray anesthetic is applied and waits for its effect to take place..
Then, with the help of a grooved probe, the tongue is raised and with a scissor (from Mayo), resting on the floor of the mouth, the cut is made to just the edge of union of the base of the tongue with the floor of the mouth.
In older children, in whom it is more difficult to achieve the required immobilization, the procedure is performed in the operating room. Anesthesia is induced (generally inhalational) and the frenulum is cut with scissors or an electrosurgical unit..
The latter has the advantage of coagulating while cutting, so it is preferable to use this technique in case of very thick braces, as it allows their complete section without subsequent bleeding..
Suturing is not required after the procedure because if it is carried out properly it will not compromise any important blood vessel.

The frenulum of the penis or frenulum of the foreskin (or preputial) is a fold of skin that joins the posterior aspect of the glans with the inner surface of the foreskin. Its usual function is to help retract the foreskin over the glans (helps the foreskin cover it) when the penis is flaccid.
However, on some occasions, this frenulum is very brief or short and restricts the movement of the foreskin, and can even cause exaggerated curvature of the penis down in erection, which is painful and makes sexual intercourse difficult..
In general, it is a very thin tissue that tears spontaneously without causing more than slight bleeding and temporary discomfort when the man begins his sexual activity..
There are, namely, two indications for performing penile frenilectomy.
It can be practiced by a pediatric surgeon, a general surgeon or a urologist, depending on each case and the age of the particular patient. Can be performed in the office with infiltrative local anesthesia.
Anesthesia is instilled and it is waited for it to take effect. A solution of continuity is created between the portion of the frenulum closest to the skin and this; a kind of tunnel.
Once this tunnel is created, both the proximal and distal portions of the frenulum are ligated with resorbable sutures and once the sutures are secured, the skin bridge that remains between them is cut..
It is an extremely quick procedure and should not cause any bleeding. In those cases of very thick and short braces (which usually bleed profusely), the same procedure is performed but in the operating room, under simple or conductive epidural anesthesia.
In these cases, the frenulum is sectioned with an electrosurgical knife to guarantee the absence of postsurgical bleeding. In the case of boys, it should always be performed in the operating room, under general anesthesia, in which case (prior consent of the parents) simultaneous circumcision is performed.



Yet No Comments