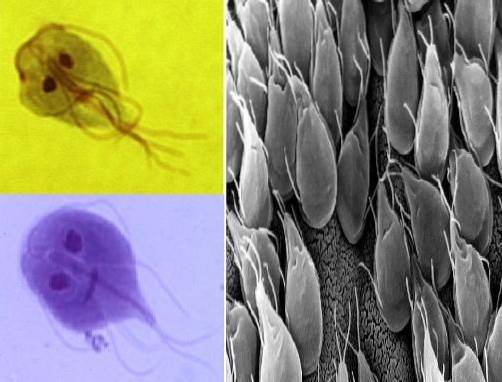
Giardia lamblia it is a cosmopolitan flagellate protozoan that causes parasitosis in humans called giardiasis. This parasitosis is one of the main causes of gastrointestinal diseases worldwide, becoming a public health problem.
Its presence is associated with a wide range of intestinal symptoms, characterized mainly by benign enteritis, but in chronic cases it can be accompanied by weight loss and malabsorption syndrome. The parasite is transmitted by fecal-oral contamination, that is, when humans ingest water or food contaminated with cysts of Giardia lamblia.
It is believed that Giardia lamblia is a zoonosis and that humans can be infected with strains of various animal species such as mammals (rodents, deer, cattle, ram, horses, dogs and cats), amphibians, reptiles, birds or fish.
Hence, the infection does not always manifest itself in the same way, that is, some strains may be more pathogenic than others. Therefore, severe, moderate or mild symptomatic cases and other asymptomatic ones are occasionally observed. Likewise, some infections can be self-limiting and others can remain chronic..
The disease is usually endemic, but epidemic outbreaks have also been described. It should be noted that the prevalence of giardiasis is three times higher in children under 10 years of age than in adults.
Of course, unsanitary conditions, contamination of water and food with fecal material and inadequate hygiene habits are the main factors that favor the proliferation of this parasite..
That is why the incidence rate always tends to be higher in populations where the socioeconomic level is low and the sanitary conditions are poor..
In addition to this, there are also certain conditions that can facilitate infection, such as decreased gastric acidity, malnutrition, and immunoglobulin A deficiency syndrome. This explains why giardiasis is less common in well-nourished and immunocompetent children..
Article index
To the protozoan Giardia lamblia It has also been known by the name of Giardia duodenalis, Giardia intestinalis or Lamblia intestinalis. However, the name that currently identifies him is Giardia lamblia.
This flagellate protozoan has a motile trophozoite form and a non-motile cystic form..
The diagnosis of this parasite is not difficult, but it must be taken into account that the fecal elimination of both trophozoites and cysts is irregular in shape. Therefore, it is recommended to do serial examinations on non-successive days.
Trophozoites are usually seen in liquid feces, in which not only their morphology can be appreciated, but also their particular movement in a falling leaf. While cysts are more common to see in stool formed.
Protist kingdom
Subkingdom: Excavata
Phylum: Metamonada
Class: Fornicate
Order: Diplomonadida
Suborder: Giardiina
Genus: Giardia
Species: lamblia
The flagellated protozoan Giardia lamblia It has two possible forms (The vegetative or trophozoite and the cystic).
The vegetative form is the one that feeds, is motile and reproduces, while the cystic form is a resistance structure, immobile and infectious.
They are pyriform or heart-shaped with bilateral symmetry. Measures 10 to 20 µm in length by 5 to 15 µm in width and 2 to 4 µm in thickness.
On the ventral side is the suction or suction disc (adherent disc), which is concave and circumscribed by a thin rim, which gives it a suction cup appearance..
The dorsal face is convex and there the lateral edges of the disc can be seen. Its cytoplasmic structures are observed in the same way on both sides of the structure, that is, its distribution is symmetrical..
In the wider limb there are 2 oval nuclei, with their respective central karyosomes, without peripheral chromatin on each side of a central axostyle, which gives it a monkey-like appearance..
From the anterior to the posterior limbs, 2 thin rod-shaped fiber shafts, called axonemes, extend. These start with 8 blepharoplasts and continue with the posterior flagella.
There are 8 flagella in total, distributed in 4 pairs: an anterior pair, a median pair, a ventral pair and a posterior or caudal pair. These organelles are responsible for the locomotion of the parasite.
The cytoplasm is uniform and finely granular. There, two curved comma-shaped bodies can be observed with certain colorations, which correspond to the Golgi apparatus and are called parabasal bodies..
The cysts are 8 to 14 µm in length and 7 to 10 µm in width. They are ellipsoid or oval in shape and have a thin, smooth, colorless membrane.
Inside they have the same structures of the trophozoite but duplicated. That is, 4 nuclei are observed, located towards one of the poles or a pair in each pole, 4 axonemes, 4 parabasal bodies and the invaginate flagella.
The karyosomes of the nuclei are smaller than in trophozoites and are eccentrically located. They do not have peripheral chromatin.
The cytoplasm tends to retract, so there is a clear space between the cyst wall and the cytoplasm. Ill-defined longitudinal fibrils are observed within the cytoplasm.
The infectious structure is represented by the cystic form.
The human ingests water or food contaminated with fecal material infested with cysts of Giardia lamblia.
Later, the parasite begins to unseat in the stomach, completing the process in the duodenum, where the cystic wall completely dissolves, becoming a tetranucleated trophozoite..
Then this structure divides, giving rise to two binucleated trophozoites under an alkaline environment. Trophozoites adhere to the intestinal mucosa through the suctory disc specifically in the villi of the duodenum and the first portions of the jejunum..
It is there where these parasites live, however trophozoites have been found in the bile ducts and in the gallbladder..
Trophozoites can move over the mucous layer at the base of the microvilli with a peculiar somersault movement..
To continue with the evolutionary cycle of the parasite, many of the trophozoites detach from the mucosa of the duodenum and are drawn into the jejunum. They remain there until dehydration of the intestinal content occurs, then passing to the colon through fecal flow..
The trophozoite retracts the flagella into the cytoplasmic sheaths, takes an oval and slightly smaller shape, surrounding itself with a cystic wall. In this way the trophozoite becomes a cyst.
Thus, they are expelled by feces to the external environment, where they can remain viable for up to two months or more, even under adverse conditions, until reaching a new host..
Mobile trophozoites that did not become encyst during fecal transit can also be expelled..
If there is not a good disposal of excreta, the faeces can contaminate water sources and food.
Likewise, non-compliance with simple hygiene habits, such as not washing hands after using the bathroom, represents a common source of contamination..
Flies can serve as mechanical transmission factors, as well as crowding and very close contacts.
On the other hand, intimate relationships that include oral-anal sex between homosexual subjects may be a possible form of transmission..
Finally, epidemics have been reported due to the seepage of sewage into adjacent drinking water systems and even in recreational freshwater spas, as chlorinated water does not destroy cysts of Giardia lamblia.
The trophozoite form is the state in which the parasite can feed, absorbing nutrients from the digestive tract.
Feeding is carried out through the dorsal surface by a process called pinocytosis (ingestion of liquid substances from intestinal contents) or phagocytosis (ingestion of solid elements from intestinal contents).
In order for the parasite to reproduce, it must be in the vegetative or trophozoite form..
The reproduction of the trophozoites of Giardia lamblia It's very simple. They reproduce asexually, that is, it occurs by longitudinal binary division.
In low or moderate parasite loads, trophozoites adhering to the intestinal mucosa can cause irritation and to a lesser extent inflammation of the mucosa of the duodenum and jejunum. Most of the time the infections can be asymptomatic.
However, acute or chronic diarrhea may develop as a result of accelerated intestinal transit related to cryptic hypertrophy, hairy atrophy, or flattening and injury of epithelial cells..
However, when the parasite load is high and the strain is virulent, several pathogenic mechanisms can be observed, among which the following can be mentioned:
The trophozoites form a mat on the duodenal and jejunal mucosa, this causes a mechanical interference of the absorption of fats, fat-soluble vitamins and sugars.
In addition, there is a deconjugation of bile salts induced by the parasite, as well as an alteration of intestinal motility and accelerated turnover of the mucous epithelium and invasion of the mucosa..
All this explains the malabsorption syndrome and weight loss in chronic cases.
Additionally, there may also be hypertrophy of the intestinal mucosa (lesion of the brush border of the microvilli) at the site of adherence by the suction disc of the parasite with or without inflammatory infiltrate (allergic or local hypersensitivity phenomenon).
Likewise, the accumulation of fat in the intestinal lumen causes diarrhea whose stools can be watery, semi-solid, greasy, bulky and foul-smelling at different times during the course of the infection..
In humans, infection by G. lamblia it is characterized by a wide spectrum of presentation. Thus, while some infected individuals present severe intestinal and general disorders, others are asymptomatic.
When symptomatic, clinical manifestations begin one to three weeks after exposure..
Giardiasis can present as enteritis that can be self-limited, manifested by diarrhea with a sudden and explosive onset. Diarrhea can become chronic and debilitating, with steatorrhea and weight loss.
There may also be abdominal cramps and general malaise without fever. Less frequently there may be nausea, vomiting, bloating, flatulence, and loss of appetite.
Diarrhea can become intermittent, lasting a few days at a time.
In chronic giardiasis in children they can cause growth retardation due to malabsorption syndrome, specifically the intestine becomes unable to absorb fats, fat-soluble vitamins, folic acid, glucose, lactose and xylose.
Finally, it should be noted that immunosuppressed people are more prone to massive infestation with severe clinical manifestations.
To diagnose parasitosis, it is necessary to observe either trophozoites or cysts in stool samples, duodenal juice or biopsy..
As the expulsion of the parasites is intermittent in the stool, a series of samples is usually requested on non-successive days to increase the probability of finding the parasite..
A direct stool exam with saline solution can be done and examined under the light microscope. This will allow to see the living trophozoites, being able to appreciate the characteristic undulating directional movement (in a falling leaf).
Lugol preparations allow better visualization of cystic forms. The Faust et al technique can be used to facilitate the concentration of cysts in samples with a low parasite load..
Permanently stained concentrates can also be made.
Through endoscopy, duodenal juice can be obtained, being a much more representative sample than feces, but requiring an invasive method..
There is a simple method called Enterotest that consists of a gelatin capsule tied to a thread, the length of the distance from the mouth to the epigastrium.
The capsule is swallowed, the parasites adhere to the thread when it is located in the duodenum, it dissolves and the thread is withdrawn. Then it is observed under a microscope.
The biopsy can be done during an endoscopy.
Another method that has been useful is the enzyme immunoassay (ELISA), to detect antigens of Giardia lamblia in the samples.
There are factors that increase the susceptibility of individuals to suffer from giardiasis. These include: strain virulence, inoculum size, achlorhydria or hypochlorhydria, and immune abnormalities.
On the other hand, there are studies that indicate that specific secretory IgA antibodies are formed in immunocompetent people. Giardia lamblia, that inhibit the binding of trophozoites to the intestinal epithelium.
Likewise, IgM and IgG antibodies are formed against trophozoites and together with complement they are capable of destroying the parasite..
The drugs of choice for giardiasis are quinacrine hydrochloride or nitroimidazoles. Among the nitroimidazoles there are:
Furazolidone is often used in pediatric patients, since it is available in liquid suspension but its cure rates are lower..
None of the drugs mentioned above can be used in pregnant women due to the risk of teratogenicity..
The only drug recommended for pregnant women is paromomycin, which, although less effective, is safer because it is not absorbed.


Yet No Comments