Haemphilus influenzae It is a gram-negative, pleomorphic coccobacillus that causes a wide variety of infections and some quite serious in humans, including meningitis, septicemia, pneumonia, epiglottitis, conjunctivitis, cellulitis or arthritis, among others. The species influenzae represents the main pathogen of this genus.
This bacterium can live as a normal microbiota in the respiratory tract of some healthy individuals. People who present this bacteria in their pharynx without having symptoms are called healthy carriers, and they are responsible for the spread of the bacteria..

The people most susceptible to serious infections by this microorganism are children and the elderly. The former are mostly affected by meningitis and the latter by pneumonia.
This bacterium belongs to the group of microorganisms called fastidious or demanding, better known as the group (HACEK) which means Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella Y Kingella.
To grow this bacterium, it is necessary to have enriched media containing factor X (hemin) and factor V (NAD or NADP). The culture medium par excellence for this bacterium is chocolate agar enriched with IsoVitaleX.
Article index
Haemophilus influenzae It belongs to the Pasteurellaceae family. It is a cosmopolitan bacterium that affects humans exclusively.
The first to isolate this bacterium was the German doctor Emil Pfeiffer, who was looking for the causative agent of the influenza epidemic that occurred in 1892. It was mistakenly thought that this microorganism was the cause of the disease, but later it was learned that the causative agent of influenza was a virus and not this bacteria.
For this reason, initially this bacterium received the following names: Pfeiffer's bacillus or Bacillus influenzae.
Some strains of Haemophilus influenzae they are capped and others are not. The capsules are typifiable according to the type of carbohydrate they have in the capsule. 6 different types are known designated by the letters a, b, c, d, e and f.
At the laboratory level, they can be differentiated by using antisera agglutinating antibodies against the corresponding polysaccharide..
Capsulated strains are pathogenic. Those of type b are the most invasive and frequently isolated in serious infectious processes. While the noncapsulated are considered habitual microbiota and, although they can also cause infections, these are not usually invasive and do not represent a greater danger.
At the laboratory level, they are difficult to isolate, as they require highly enriched media for optimal development, such as chocolate agar or Levithal agar..
That is why this microorganism belongs to the group of bacteria called demanding from the nutritional point of view, although some authors prefer to call them annoying microorganisms..
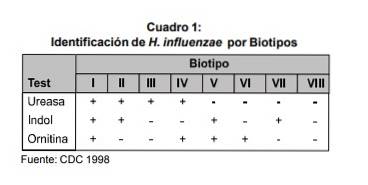
Its reaction to catalase and oxidase tests is positive. It is a facultative aerobic and anaerobic microorganism that grows well at 35-37 ° C, at pH 7.6 and with 5% COtwo. From a biochemical point of view, this bacterium is classified into 8 biotypes as proposed by Kilian.
The classification is based on the results of certain tests, such as indole, ornithine and urease..
Haemophilus influenzae it is very similar to the rest of the species of the genus Haemophilus, since they are very small coco bacilli and their size ranges between 0.2-0.3 µm wide and 0.5-0.8 µm long.
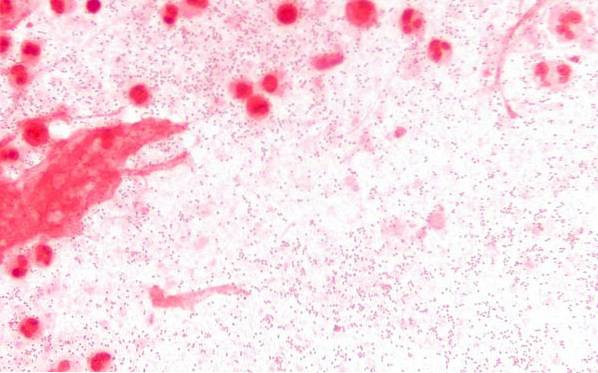
However, the Haemophilus influenzae Seen under the microscope they are very pleomorphic, that is, they can take different forms. These can be seen as very short bacilli (coccobacilli) or slightly more elongated bacilli, and even filamentous. With the Gram stain they stain red, that is, they are Gram negative.
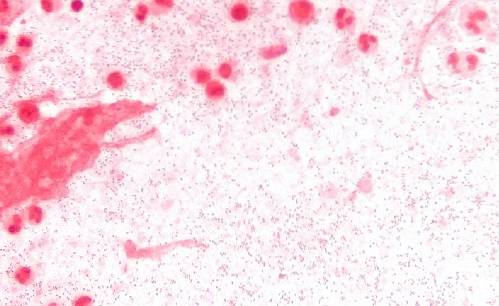
Morphologically they are very similar to the genus Pasteurella, but the latter have a bipolar coloration that differentiates them. They are not spore formers. They also do not have flagella, therefore they are immobile..
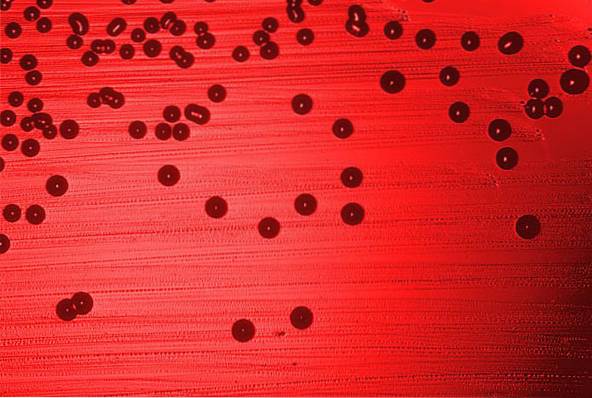
After a 24-hour incubation on chocolate agar, very small, convex colonies of 0.5 to 0.8 mm in diameter develop, granular in appearance, transparent and opaque..
At 48 hours of incubation, the colonies have grown somewhat more (1 to 1.5 mm). It should be noted that the colonies of the strains that have capsules tend to be more mucoid and much larger, measuring up to 3.0 mm..
Strains of Haemophilus influenzae 50-75% colonize the nasopharynx of healthy children and adults. It is also possible to find this strain in the genital tract of some individuals..
Haemophilus influenzae It is a pathogenic bacterium exclusive to humans, whose natural habitat is represented by the upper respiratory tract of the human being. There the bacteria can grow and thrive without causing harm to the host..
Reproduction is asexual by fission, in this type of reproduction, an organism first duplicates its genetic material, then forms two new cells from an original stem cell.
The term Haemophilus is a compound word, it comes from two Greek words, 'haemo', which means blood and 'philus', which comes to be affinity.
This bacterium lives up to its name, as it grows extremely well on warmed blood agar (chocolate agar). It can also grow on blood agar, but needs to be in the company of a strain of S. aureus. The latter, being beta-hemolytic, breaks down erythrocytes and releases the factor V that Haemophilus needs..
This is how the colonies of Haemophilus can develop near the strain of S. aureus. This phenomenon is known as satelliteism and is frequently used as a diagnostic strategy..

It should be noted that the strain of Haemophilus influenzae does not produce hemolysis on blood agar, which differentiates it from other species of Haemophilus, such as the H. haemolyticus Y H. parahaemolyticus.
This microorganism is transmitted by secretions, mainly respiratory secretions (saliva and mucus) emitted by sick people or carriers of the bacteria..
Bacteria travel in secretions expelled when the patient sneezes or coughs. Bacteria spread in the environment and are inhaled by the susceptible individual.
Haemophilus influenzae it is a pyogenic microorganism, which is why it generates purulent secretions.
Among the main pathologies that it causes are meningitis, septicemia, pneumonia, epiglottitis, conjunctivitis and otitis, among others.
When bacteria enter the bloodstream, it is called bacteremia and is the crucial step for the spread of the microorganism to other organs or tissues. When the microorganism multiplies in the blood it is called septicemia, this condition compromises the general condition of the patient.
Meningitis is a serious disease that causes a stiff neck, headache, vomiting or changes in behavior, in some cases leading to death. This infection is common in children.
It presents as a serious complication of a previous respiratory tract infection, such as bronchitis or acute febrile tracheobronchitis. It presents with a high fever, dyspnea, or a productive cough with purulent sputum. It can coexist with bacteremia. This affectation is more common in older adults.
Conjunctivitis presents with redness of the conjunctiva, burning, swelling of the eyelids, presence of purulent discharge or hypersensitivity to light (photophobia).
It is an infection of the paranasal sinuses that causes nasal congestion and abundant discharge. The discharge may be liquid or thick, greenish or yellowish, and with or without blood. Other symptoms include: cough, fever, sore throat, and swollen eyelids. This affectation is generally caused by noncapsulated strains..
It presents with a strong and sudden sore throat, fever, muffled voice or inability to speak, drooling, among other signs. This occurs due to obstructive laryngeal edema caused by the infection. Can cause death by suffocation.
The best way to make the diagnosis is through culture. The sample will depend on the infectious process.
If meningoencephalitis is suspected, a sample of cerebrospinal fluid should be taken by lumbar puncture for cytochemical study and culture. In the event of septicemia, blood samples will be taken to perform a series of blood cultures..
If the process is conjunctivitis, secretion emitted by this mucosa will be taken. In case of pneumonia, a sample of sputum or bronchial lavage is cultured.
The samples are seeded on chocolate agar and incubated aerobically with 5% CO.two for 48 hours of incubation.
Identification can be carried out using manual biochemical tests or also by automated systems such as the VITEK 2.
Serotyping is carried out through the agglutinating antisera. Strains of Haemophilus influenzae that do not react to any antiserum are classified as non-capsulated or nontypeable.
Levithal Agar distinguishes between capsulated and non-capsulated strains.
Haemophilus influenzae It can be treated with beta-lactams, such as ampicillin, ampicillin / sulbactam, amoxicillin / clavulanic acid, piperacillin / tazobactam. Third-generation cephalosporins, such as: ceftriaxone, cefotaxime, and cefoperazone, or carbaperazone, are usually used in severe infections.
It is important to note that ampicillin is no longer being used because currently most of the isolated strains are resistant to this antibiotic, due to the production of a beta-lactamase.
Macrolides and quinolones can also be used.
However, the most advisable thing is to perform the antibiogram and place treatment according to the reported sensitivity..
After the introduction of the vaccine against Haemophilus influenzae type b the decrease in cases of meningitis due to this microorganism decreased significantly.
Currently, the capsular antigen type b (polyribosyl-ribitol-phosphate) of the H. influenzae It is included in the pentavalent vaccine that also prevents against diphtheria, tetanus, pertussis and hepatitis B.
The vaccine is given in 3 or 4 doses. The 4-dose schedule is as follows:
The first dose is started at 2 months of age. Then two more doses are given every two months (that is, at 4 and 6 months of age). Finally the fourth dose is placed 6 or 9 months after placing the third. The last dose represents the boost.
The vaccine is contraindicated in:
- Patients who have had a severe anaphylactic (allergic) reaction against the components of the vaccine.
It is important not to confuse side effects with an anaphylactic reaction. Anaphylactic reactions are serious immune responses that compromise the life of the patient. While, the adverse effects can be local redness at the puncture site and fever.
- It is also contraindicated in patients who are sick or have low defenses. In these cases, it is necessary to wait for normal conditions to recover to be able to administer the vaccine..
- Finally, vaccination is not recommended in children under 6 weeks of age..

Yet No Comments