
The Sokolow index It is a criterion used to diagnose the enlargement of the left ventricular cavity of the heart, from the measurement of the waves that represent the left ventricle in the electrocardiogram.
The electrocardiogram is a non-invasive study that graphically represents the electrical activity of the heart. It is widely used as it is inexpensive, easy to use and provides important information on the patient's cardiac health status.
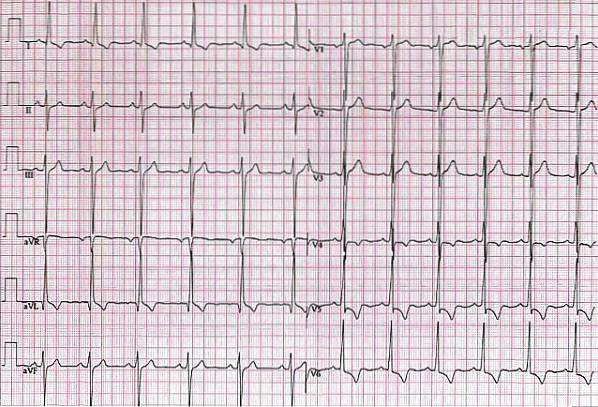
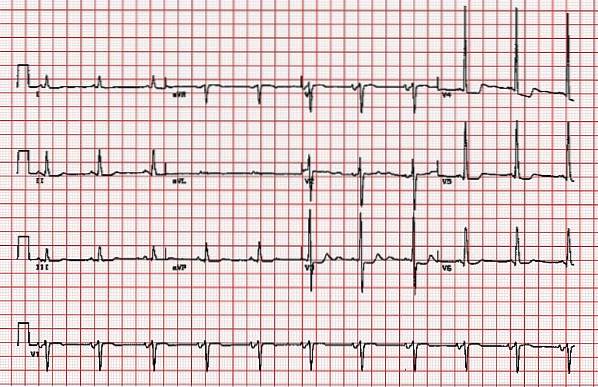
The electrocardiogram is printed on a millimeter sheet. From the sum of the small squares that the amplitude occupies a wave, the voltage of the same is obtained. The Sokolow index is the result of the sum of the amplitude of the S wave, in the precordial vectors V1 plus the R wave in V5 or V6. Thus: S V1 + R V 5 or 6 = Sokolow index.
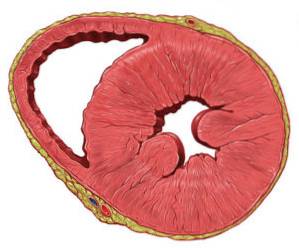
A result greater than 35 mm indicates that the patient has left ventricular hypertrophy, that is, their left ventricular heart chamber is thicker than normal..
This type of anomaly is a consequence of diseases such as arterial hypertension, which overloads the activity of the heart muscle due to the high pressures it must overcome to pump blood.
Article index
The North American cardiologists Maurice Sokolow and Thomas Lyon, based their professional careers on the study of arterial hypertension and its complications.
One of the most frequent morbidities associated with this disease is left ventricular hypertrophy, which is nothing more than the thickening of the muscular wall of the left ventricle of the heart..
These specialists described a way to calculate the state of the heart muscle, through the measurement of the voltage of some waves in the electrocardiogram. The technique was published in 1949 in the scientific journal American heart journal and it was titled "The ventricular complex in left ventricular hypertrophy obtained by unipolar precordial and limb electrodes".
The method is named Sokolow-Lyon index, and it is one of the criteria currently used to determine left ventricular hypertrophy in patients with heart disease, especially those with high blood pressure.
The electrocardiogram is a non-invasive and painless study which gives an objective result of the cardiac electrical activity.
To do this, 10 devices called electrodes are placed. 6 of them go to specific points on the chest and the other 4 go to the wrists and ankles. The precordial electrodes (V) are arranged as follows:
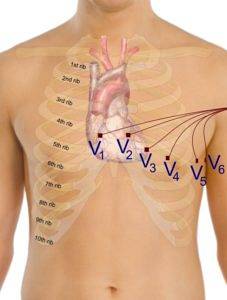
1: fourth intercostal space to the right of the sternum.
2: fourth intercostal space to the left of the sternum.
3: at the midpoint of the line connecting V2 to V4.
4: at the junction of the fifth intercostal space with the midclavicular line.
5: parallel to V4 but on the anterior axillary line.
6: parallel to the previous ones, but in the mid axillary line.
In this study, time, expressed in seconds, is measured in the horizontal plane. While the voltage, expressed in volts, in the vertical plane.
Therefore, on the graph paper where the electrocardiogram is printed, a 1 mm square on the horizontal plane represents 0.04 seconds and 0.1 millivolts on the vertical plane.
By international convention, the first wave that appears in the electrocardiogram is called p wave y represents the state of atrial depolarization.
Ventricular depolarization, that is, the electrical activity of the ventricle, is represented by the so-called QRS complex where Q translates the depolarization of the ventricular septum; R is a positive wave that indicates the depolarization of the ventricular muscle and S is a negative wave that represents the late depolarization of the ventricle..
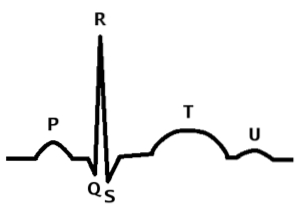
After this complex, a positive wave of low amplitude is observed, the t wave, indicating repolarization of the ventricle.
Knowing these parameters and their normal values, any abnormality of the cardiac electrical system can be inferred just by studying the electrocardiogram in depth..
Doctors Sokolow and Lyon were pioneers in implementing the measurements of the amplitude of the waves that reflect the state of the left heart, to diagnose anomalies in this region.
The measurement technique proposed by them consists of adding the S wave in V1 with the R wave in V5 or V6. This result should be less than 3.5 mV or 3.5 mm. A result greater than this value indicates an increase in the thickness of the left ventricle, which is pathological in a patient with arterial hypertension..
The Sokolow-Lyon index very accurately diagnoses left ventricular hypertrophy, reaching up to 92% specificity. The problem is that its sensitivity reaches only 25%.
This means that it is very likely that it will interpret false negatives, identifying as healthy patients who actually have a hypertrophy of the ventricle in its initial stages.
The low sensitivity of the index is explained by the fact that when the study was carried out in 1949, the subjects evaluated were untreated hypertensive with very advanced disease. Therefore they had obvious hypertrophy.
Currently other criteria are used, together with the Sokolow index, to identify patients with left ventricular thickening. One of the most used is the Cornell index, in which measurements are adjusted for sex..
The Sokolow index demonstrated that the electrocardiogram is a tool that can provide diagnostic data for serious morbidities of important diseases such as arterial hypertension.
The gold standard for detecting ventricular hypertrophy is the echocardiogram. However, this study is expensive and requires trained personnel to perform and analyze it..
The importance of the Sokolow index is that it is based on the measurement from the electrocardiogram, which is a basic study of the clinical examination, it is also inexpensive, easy to perform and can be analyzed by any general practitioner.
From the electrocardiogram, the doctor makes the diagnostic approach to ventricular hypertrophy and this patient will be referred to the cardiologist to be studied in depth.


Yet No Comments