
Contents
The word "dementia" describes a set of symptoms that can include memory loss and thinking difficulties, problems with problem solving or language. These changes are usually small, but for someone with dementia it means that they have become severe enough to affect daily life. A person with dementia may also experience changes in their mood or behavior.
50% of dementias are due to Alzheimer's disease. This, like other cortical dementias, affects the functions supported by the cortex, such as memory (amnesia), language (aphasia), and perceptual and manipulative abilities (agnosia and apraxia)..
In general, primary dementias, such as Alzheimer's, are often irreversible. There are some diseases, however, that lead to treatable and reversible dementias. This is the case of dementias associated with metabolic and deficiency diseases (hepatic encephalopathy or vitamin B-12 deficiency, for example), drug or metal poisoning, or infectious diseases, such as encephalitis or meningitis.
Alzheimer's disease is the most common form of dementia, affecting up to 70% of all people with dementia.
This disease was first described in 1907 by Dr. Alois Alzheimer with the case of Auguste Deter, a middle-aged woman with dementia and specific changes in her brain. For the next 60 years, Alzheimer's disease was considered a rare condition that affected people under the age of 65. It wasn't until the 1970s that Dr. Robert Katzman declared that "senile dementia" and Alzheimer's disease were the same disorder and that it was not a normal part of aging..
Alzheimer's disease is associated with age and affects approximately 10% of the population over the age of sixty-five, its prevalence increasing to 50% in people over the age of eighty-five. Life expectancy once diagnosed is between five and ten years.
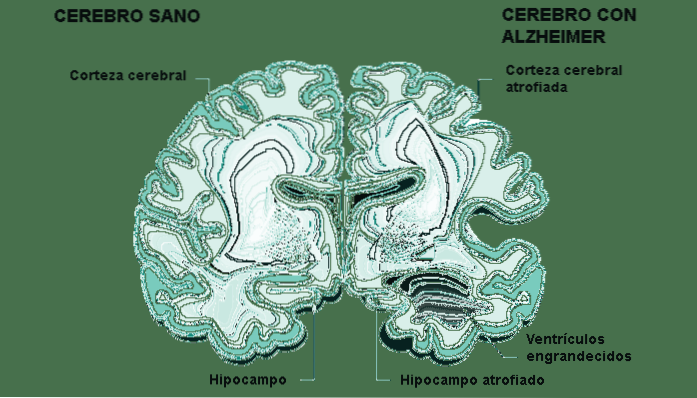
Dr. Alzheimer examined the brain of his patient Ms. Deter after her death and observed a significant reduction in the outer layer of the cerebral cortex, a region involved in memory, language, and judgment. He also found two types of deposits in Deter's brain, some were plaques known as senile plaques and the other type of deposit was brain cells known as neurofibrillary tangles. These plaques damage synapses, so signals cannot pass between brain cells. Tangles kill brain cells by preventing the normal transport of food and energy around the brain cell..
Distribution of senile plaques and neurofibrillary tangles in advanced stages of Alzheimer's disease.
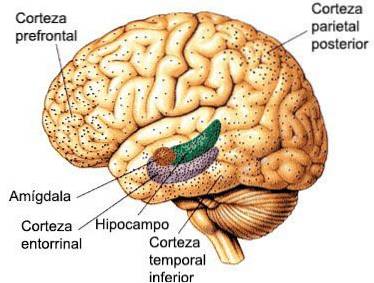
The outer part of the brain is usually the area affected first by the disease. Short-term memory loss is therefore one of the first symptoms of Alzheimer's disease. But as the disease progresses to deeper parts of the brain, long-term memory is also lost. The disease also affects many of the other functions of the brain and consequently many other aspects of behavior are affected..
These pathological changes are first observed in the hippocampus and the parietal association cortex, and progressively spread throughout the cortex and the rest of the brain..
Subsequently, a significant loss of cholinergic neurons also appears in the basal forebrain, especially in the nucleus basalis of Meynert..
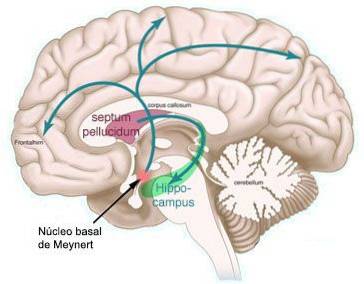
At the same time, decreased levels of norepinephrine, serotonin, and somatostatin (a neuropeptide) are observed in the frontal lobe, occipital lobe, and hippocampus..
The causes of the disease are being investigated, which surely include factors in the environment, biochemical alterations and immune processes. It is something that can vary from person to person and can be due to one factor or several factors. However, some genes that could be involved in the same family have been located. For example, a gene has been located on chromosome 21 that codes for an aberrant precursor of the b-amyloid protein of senile plaques. Likewise, genes involved in other family forms of the disease have also been located on chromosomes 14 and 1. A genetic marker that increases the risk of Alzheimer's disease is the presence of allele 4 in the alipoprotein E gene, located on chromosome 19. This protein is related to lipid metabolism, and has an affinity for the b-amyloid protein of senile plaques. The presence of an allele 4 triples the chances of suffering from Alzheimer's disease, and the presence of two alleles 4 ensures that you will suffer from Alzheimer's disease from the age of eighty.
In the early stages, the symptoms of Alzheimer's disease can be very subtle. However, it often begins with memory lapses and difficulty finding the right words for everyday objects..
Other symptoms can include:
Symptoms vary and the disease progresses at a different rate depending on the individual and the areas of the brain affected. A person's abilities can fluctuate from day to day, or even within the same day, worsening in times of stress, fatigue, or poor health..
Unfortunately, there is currently no effective treatment for Alzheimer's disease. Patients are often treated symptomatically, with neuroleptics, antidepressants, anxiolytics ... Drugs that increase cholinergic neurotransmission are also used, since it is assumed that memory loss is due in part to the involvement of this neurotransmission system. Inhibitors of acetylcholinesterase, the enzyme that breaks down acetylcholine in the synaptic space, are commonly used..
Other important characteristics of Alzheimer's disease are anosognosia, or ignorance of the cognitive deficit on the part of the sufferer, changes of character, with an increase in irritability and / or apathy and lack of initiative, affective disorders, such as anxiety and depression, and sometimes psychotic symptoms, such as delusions and / or hallucinations.
Lewy body dementia is a progressive brain disorder in which Lewy bodies (abnormal deposits of a protein called alpha-synuclein) accumulate in areas of the brain that regulate behavior, cognition, and movement..
It is a complex disease that can present with a variety of symptoms that include problems with thinking, memory, movement, sleep and / or changes in behavior, among other physical, cognitive and behavioral symptoms..
It also affects autonomic bodily functions, such as blood pressure control, temperature regulation, and bladder and bowel function. Progressively debilitating, this disease can cause people to experience visual hallucinations or act out their dreams.
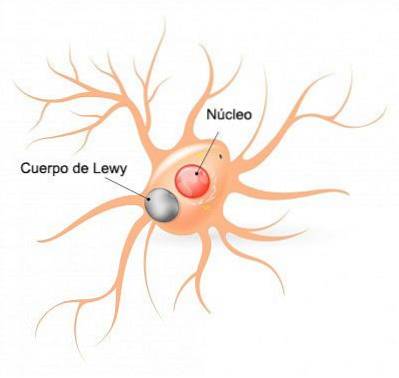
It is characterized by the appearance of Lewy bodies and occasionally senile plaques as well. Lewy bodies are located in the cortex, and are also seen in subcortical structures, such as the substantia nigra.
Lewy body disease has symptoms that can closely resemble other diseases such as Alzheimer's and Parkinson's, making it sometimes difficult to diagnose.
Pick's disease
Pick's disease is a type of dementia similar to Alzheimer's, but much less common. It is also a type of disorder known as frontotemporal dementia or frontotemporal lobar degeneration..
Pick's disease is a rare type of age-related dementia that affects the frontal lobes of the brain. It affects the parts of the brain that control emotions, behavior, personality, and language, causing speech problems such as aphasia, behavioral difficulties, and eventually death. It was first described by the Czech neurologist and psychiatrist Arnold Pick in 1892. In some earlier medical texts, Pick's disease is used interchangeably with "frontotemporal dementia.
Our brain uses a transport system to help carry the nutrients it needs from one place to another. This system is made of proteins that guide nutrients where they need to go. With Pick's disease, proteins do not work as they should.
It can sometimes be confused with atypical forms of Alzheimer's disease, but it has different characteristics:
It is characterized by mood and affective disorders, and behavioral changes, and pseudopsychopathy and / or pseudo-depression may appear. Disinhibition is observed, with hyperorality (change in eating habits and introduction of inedible objects in the mouth) and hypersexuality (with absence of discrimination due to age, sex or degree of relationship with the person). Exhibitionistic behavior and significant obsessive-compulsive traits may also appear. The patient is anosognotic. Memory, language, and executive functions are often impaired.
Those affected by Pick's dementia may exhibit socially inappropriate behaviors, such as urinating in public or explicit sexual comments. An increase in sexual activity and strange behaviors, such as masturbation in public, may appear. Their eating habits are disturbed, they gain weight very quickly, or they try to eat inedible things (plaster, feces, or spoiled food). They tend to be unconcerned with economic issues and progressively isolate themselves from their social environment, also losing language skills, ending in silence..
There are cerebral degenerations that affect only one or two cerebral lobes, and that, therefore, have an exclusive symptomatology of the functions carried out by the affected cerebral lobes.
One of them is slowly progressive aphasia, which results from a degeneration of the perisylvian region of the left hemisphere. The lesion focused on the right parietal lobe is known as slowly progressive apraxia, and mainly affects constructive practices and spatial perception. Finally, posterior cortical atrophy, affecting the parieto-occipital cortices, has also been described. Although histologically they appear to differ from Alzheimer's or Pick's dementias, it is not clear if they are only the first phase of generalized cortical dementia.



Yet No Comments