
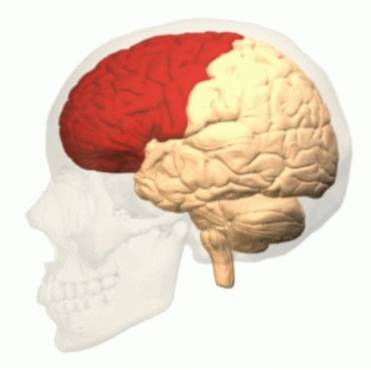
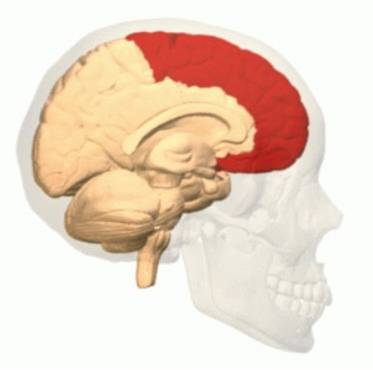
The frontal lobe it is the largest lobe of the four that exist in the mammalian brain. It is located in the front part of each brain hemisphere and controls important cognitive functions, such as emotional expression, memory, problem solving, language, impulse control, social and sexual behavior, spontaneity or muscle control. The left frontal lobe affects the muscles on the right side of the body, and the right frontal lobe controls the muscles on the left side of the body.
The frontal lobe is the brain area that most distinguishes humans from other animals. For this reason, it has aroused special interest in researchers, who have carried out multiple studies on its functions and its operating mechanism..
This region is widely related to functions as important as language, control of motor actions and executive functions, so that, if injured, the person can suffer serious problems that we will also talk about in this article..
Article index
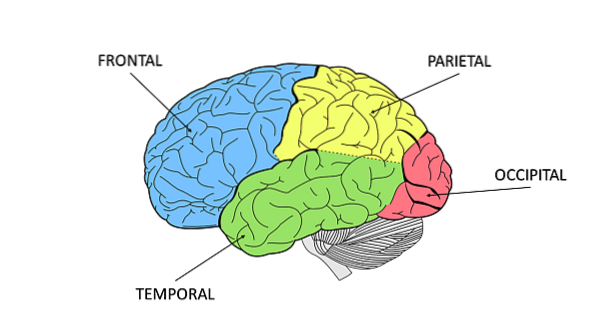
The brain is made up of cortical areas and subcortical structures. The cerebral cortex is divided into lobes, separated by furrows, the most recognized are the frontal, the parietal, the temporal and the occipital, although some authors postulate that there is also the limbic lobe.
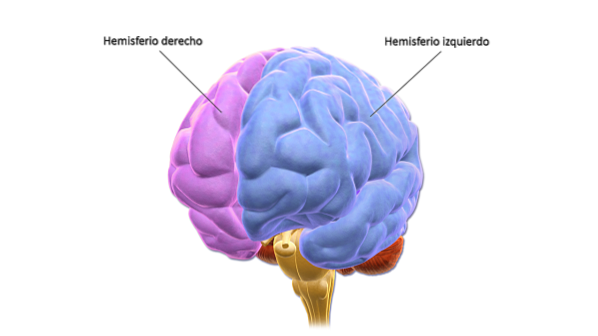
The cortex is in turn divided into two hemispheres, the right and the left, so that the lobes are present symmetrically in both hemispheres, with a right and a left frontal lobe, a right and left parietal lobe, and so on..
The cerebral hemispheres are divided by the interhemispheric fissure while the lobes are separated by different sulci.
The frontal lobe reaches from the most anterior part of the brain to the Rolando fissure (or central fissure) where the parietal lobe begins and, on the sides, to the Silvio fissure (or lateral fissure) that separates it from the temporal lobe.
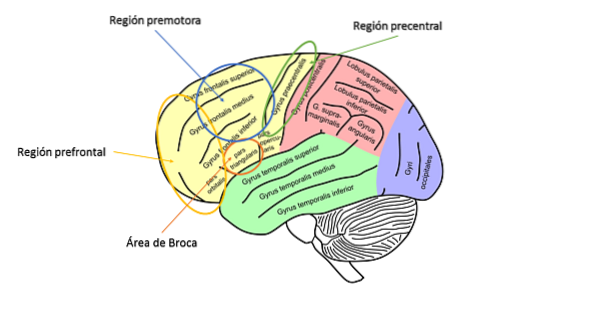
Regarding the anatomy of the human frontal lobe, it can be said that it is very voluminous and has the shape of a pyramid. It can be divided into precentral and prefrontal cortex:
It is composed of the primary motor cortex (Brodmann's area 4), the premotor cortex, and the supplementary motor cortex (Brodmann's area 6). This area is basically motor and controls the phasic movements of the body (programming and initiation of movement), as well as the movements necessary to produce language and posture and body orientation..
It is the association zone, it is made up of the dorsolateral, ventrolateral and orbitofrontal cortex, and its functions are related to the executive system, such as the control and management of executive functions.
The frontal lobe, and especially the prefrontal cortex, is the cortical area most widely connected to the rest of the brain. The main connections are as follows:
Receive and send information to the rest of the lobes. The most important are the frontotemporal connections, which are related to audioverbal activity and the frontoparietal ones, related to the control and regulation of cutaneous-kinesthetic sensitivity and pain.
They facilitate emotional and affective regulation through neuroendocrine and neurochemical secretions.
In these circuits some sections of the frontal lobe are connected with the striatum, the globus pallidus and the thalamus:
You could say that the frontal lobe receives inputs of the areas responsible for the sensory processing of information and sends outputs to the areas in charge of giving an answer, especially motor.

The prefrontal cortex is the last area to develop in the frontal lobe and the brain in general. This area is especially important because it fulfills functions without which we would not be effective in our daily lives, such as planning and organizing future behaviors.
It is shaped like a pyramid, like the frontal lobe, and has an inner, outer, and inner face. Regarding the connections it establishes with the rest of the structures, there are three main circuits:
It goes to the dorso-lateral area of the caudate nucleus. From here it connects with the dorso-medial globe pallidus and with the substantia nigra. These project to the dorso-medial and ventral-anterior thalamic nuclei, and from there return to the prefrontal cortex.
It projects to the ventromedial caudate nucleus, then to the globe pallidus and the ventro-medial substantia nigra, from there it passes to the ventral-anterior and dorso-medial thalamic nuclei and finally returns to the prefrontal cortex.
It projects to the ventral striatum, it has connections with the globe pallidus, the ventral tegmental area, the habenula, the hypothalamus, and the amygdala. Finally it returns to the prefrontal cortex.
This area is attributed the functions of structuring, organizing and planning behavior. The patient suffers the following faults if this area is injured:
The frontal lobe fulfills multiple functions that can be summarized as:
Executive functions will be described in greater depth below due to their great importance in humans..
Executive functions could be defined as the last step in the control, regulation and direction of human behavior. This concept arises for the first time from the hand of A.R. Luria in 1966 in his book Higher Cortical Function in Man.
Lezak popularized this term in American psychology. This author highlights the difference between executive and cognitive functions, stating that, although cognitive functions suffer damage if executive functions function correctly, the person will continue to be independent, constructively self-sufficient and productive.
Executive functions are made up of four components:
It is the process by which needs are determined, what is wanted and what is capable of getting what is wanted. If a person has this function altered, they cannot think what to do and have difficulties in starting activities.
These alterations can occur without the need for brain damage, simply with a poor organization in the prefrontal lobe.
It is responsible for determining and organizing the necessary steps to carry out an intention.
This process requires certain capacities such as: conceptualizing changes in present circumstances, seeing herself developed in the environment, seeing the environment objectively, capable of conceiving alternatives, making choices and developing a structure to carry out the plan.
It is interpreted as the action of initiating, maintaining, changing and for sequences of complex behaviors in a comprehensive and orderly manner.
It is the assessment based on the objectives and the resources used to achieve those objectives.
The teaching system is very important for the correct configuration of executive functions, since these functions begin to develop in childhood, from the first year of life, and do not mature until puberty or even later..
Executive functions are mainly related to the prefrontal cortex, but some studies performed with PET (positron emission tomography) indicate that, when the activity becomes routine, another part of the brain takes over in the activity to free the patient. prefrontal cortex and that it can take care of other functions.
The most used techniques for the evaluation of the executive system are:
The frontal lobe can be damaged as a result of trauma, heart attacks, tumors, infections or due to the development of some disorders such as neurodegenerative or developmental disorders.
The consequences of frontal lobe damage will depend on the area damaged and the extent of the injury. The syndrome, due to damage to the frontal lobe, better known is the prefrontal syndrome that will be described below.
The first well-documented description of a case of this syndrome was that made by Harlow (1868) on the case of Phineas Gage, over time this case has continued to be studied and today it is one of the best known in the field. of psychology (cited in León-Carrión & Barroso, 1997).

Phineas was working on a train track when he had an accident while compacting gunpowder with an iron bar. It seems that a spark reached the gunpowder and it exploded, throwing the iron bar directly at his head. Phineas suffered an injury to the left frontal lobe (specifically in the medial orbital region) but he was still alive, although he had sequelae.
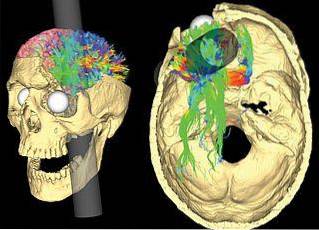
The most significant changes due to the injury suffered were increased impulses, inability to control oneself, and difficulties planning and organizing..
People with injured prefrontal cortex present changes in personality, motor skills, attention, language, memory and executive functions.
According to Ardila (cited in León-Carrión & Barroso, 1997) there are two ways or aspects to describe the changes in personality caused by this syndrome:
Among the changes in motor skills we can find:
The main changes occur in the orientation response, patients have deficits to orient themselves to the stimuli that they should at home and when following the examiner's instructions..
The most characteristic are:
The frontal lobes play an important role in memory, especially in short-term memory. Patients with frontal lobe lesions have problems with memory storage and retention. The most frequent alterations are:
Executive functions are the most impaired in patients with frontal injuries since for their correct performance a complex elaboration and the integration and coordination of various components are necessary..
People with frontal syndrome are unable to form a goal, plan, carry out actions in an orderly manner, and analyze the results obtained. These deficits prevent them from leading a normal life since they interfere with their work / school, family, social tasks ...
Although the symptoms described are the most common, their characteristics are not universal and will depend both on patient variables (age, premorbid execution ...), as well as on the lesion (specific location, magnitude ...) and the course of the syndrome..
The category of frontal syndromes is very broad and includes another series of syndromes that differ according to the injured area. Cummings (1985), describes three syndromes (cited in León-Carrión & Barroso, 1997):
Imbriano (1983) adds two more syndromes to the classification elaborated by Cummings (cited in León-Carrión & Barroso, 1997):



Yet No Comments