
The lissencephaly neurological disorder in which there is insufficient development of the cerebral sulci and convolutions. It is a congenital malformation product of a neuronal migration disorder, that is, in the process that nerve cells follow from the place of origin to their final location in the cerebral cortex during the embryonic period.
The clinical course of lissencephaly can include generalized growth retardation, muscle spasms, seizures, severe psychomotor retardation, facial abnormalities, among others. In addition, this type of neuronal migration disorder is often associated with other medical conditions, such as Miller-Dieker syndrome and Walker-Warburg syndrome..
There is currently no curative treatment for lissencephaly. The prognosis for those affected by this pathology varies considerably between different cases, depending on the degree of brain malformation. Some will not survive to 10 years of age, others may show severe developmental and growth retardation, and others near normal physical and cognitive development.
Article index
Lissencephaly is a genetic brain malformation characterized by the absence of normal convolutions in the cerebral cortex. The cerebral convolutions or gyri are each one of the existing folds on the outer surface of the brain, separated from each other by a series of furrows called cerebral fissures or fissures..
Specifically, lissencephaly can manifest with different degrees of involvement, characterized by the absence (agiria) or reduction (pachyria) of the cerebral convolutions.
Agiria refers to the absence of folds on the brain surface and is often used as a synonym for "complete lissencephaly", while pachyria or the presence of few thicker folds is used as a synonym for "incomplete lisecephaly".
Thus, lissencephaly results from a disorder of brain development resulting from a group of abnormalities in neuronal migration. When the nervous system is forming and developing during the prenatal stage, neurons must travel from the primitive layers or areas to the cerebral cortex..
During embryonic growth, newly formed cells that will later become specialized nerve cells must migrate from the surface of the brain to a preprogrammed final location. This migration takes place in successive moments from the seventh week of gestation to the twentieth.
There are various mechanisms by which neurons reach their final location: some reach their location through movement along glial cells, while others do so through mechanisms of chemical attraction.
The ultimate goal of this displacement is to form a 6-layer laminar structure in the cerebral cortex, essential for the proper functioning and development of cognitive functions..
When this process is interrupted and lisecephaly develops, the cerebral cortex presents an abnormally thick structure of 4 poorly organized layers.
Therefore, at the anatomical level, lissencephaly can be defined by the presence of agiria or pakyrie and even the formation of a double cortex (heterotopia).
Lissencephaly is a group of rare brain malformations. Although there are no statistical data on the prevalence of the milder forms of lissencephaly, the classic form has a frequency of 11.7 per million newborn infants.
The absence of recent data is mainly due to the sporadic appearance of this pathology, as well as the fact that a good part of the cases remained undiagnosed due to the absence of technical doctors.
However, currently the use of advanced neuroimaging techniques in neurological evaluations has allowed a precise recognition of this pathology and therefore an increase in diagnosed cases.
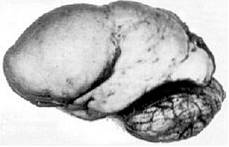
Lissencephaly is a neurological disorder characterized by producing a completely or partially smooth brain surface, and therefore a paucity of development of brain gyrus and grooves..
The classic forms are associated with the presence of an abnormally thick cerebral cortex composed of 4 primitive layers, a mixture of agiria and pachyria, neuronal heterotopia, dilated and dysmorphic cerebral ventricles, and in many cases with hypoplasia of the corpus callosum.
In addition to these characteristic anatomical findings, affected individuals may also present with other associated brain malformations, such as microcephaly..
All structural alterations will produce a wide range of symptoms and medical signs:
There is a wide variety of classifications of lissencephaly based on pathologic, genetic, and anatomical findings. Despite this, one of the most common classifications is the one that refers to type I and type II of lissencephaly:
It is a sporadic type in which the cortex has a certain organization, although it is made up of fewer layers than usual, generally 4 layers.
It is characterized by an unstructured cerebral cortex in which no layer can be recognized (polyrogyric) that develops with severe muscle changes, neurological dysfunction, hydrocephalus and encephalocele.
In addition to this, there are other classifications based on the associated malformations and the etiological cause. Based on these criteria, lissencephaly can be classified into:
Research that has tried to find the specific causes of lissencephaly indicate that there may be genetic and non-genetic etiological factors: intrauterine infection; cerebral ischemia or deficient oxygen supply to the brain during fetal development; alteration or absence of a region of chromosome 17; X-linked autosomal recessive transmission.
The causes of this pathology are heterogeneous, approximately 76% of the diagnosed cases present primary genetic alterations, while the rest of the cases present some association with another series of environmental factors.
It is generally considered that lissencephaly is a fundamentally genetic pathology associated with different alterations in some of the following genes: LIS1, 14-3-3, DCX, REELIN and ARX.
On the other hand, scientific evidence suggests that in isolated cases of lissencephaly, this pathology can result from the presence of mutations in at least two different genes:
In the case of the LIS1 gene, such mutations may occur sporadically at random or may result from chromosomal rearrangements from one of the parents. On the other hand, in the case of the XLIS gene, mutations can also occur randomly in the absence of a family history and in other cases it appears as an inherited condition linked to the X chromosome..
Lissencephaly, in addition to presenting in isolation, showing the structural alterations and clinical symptoms characteristic of this pathology, may appear associated with other genetic diseases:
This pathology results from a mutation in a gene located on chromosome 17p13. At the cynical level, it is characterized by the presentation of classic lissencephaly, facial abnormalities, severe developmental disorder, epilepsy, or eating problems..
This pathology is a congenital form of muscular dystrophy that is associated with the presence of brain and neck abnormalities. At a clinical level, Walker-Warburg syndrome is characterized by the presence of type II lisecephaly, hydrocephalus, hypoplasia of the brain stem and cerebellum, generalized muscular hypotonia, absence or poor psychomotor development, ocular involvement and convulsive episodes.
Lissencephaly can be diagnosed before birth, approximately at the end of the second trimester, since it is from that moment when the cerebral convolutions are visible on ultrasound scans..
The ultrasound techniques that are used routinely in the santal controls of the pregnancy, can indicate the presence of alterations and brain abnormalities, however, they should be complemented with other diagnostic techniques.
When there is an ultrasound suspicion of lissencephaly, other types of secondary examinations should be used, such as magnetic resonance imaging or genetic studies to detect possible alterations..
In addition to this diagnostic route, when there is a compatible family history or a history of lissencephaly, it is possible to perform other types of tests such as amniocentesis (extraction of amniotic fluid that surrounds the fetus) and chorionic villus sampling (extraction of a sample of tissue from an area of the placenta) to identify the presence of genetic abnormalities.
Despite this, it is more common for the diagnosis of lissencephaly to be made after birth through the use of computed tomography or magnetic resonance imaging..
There is no curative intervention for lissencephaly, it is a pathology that cannot be reversed.
The treatments used are aimed at improving the associated symptoms and secondary medical complications. For example, the use of gastrostomy to overcome feeding difficulties, surgical bypass to drain a possible hydrocephalus, or the use of antiepileptic drugs to control possible seizures.
Therefore, the usual treatment for lissencephaly is directed towards the specific symptoms that appear in each case and requires the coordinated effort of a large team of specialists: pediatricians, neurologists, etc..
The medical prognosis of an individual suffering from lissencephaly depends fundamentally on the severity of this.
In the most severe cases of lissencephaly, the affected person may not be able to develop physical and cognitive skills beyond those of a child between the ages of three and five months..
In general, severely affected children have a life expectancy of approximately 10 years. The most common causes of death being aspiration or drowning with food or liquids, respiratory diseases or seizures.
On the other hand, there are cases of children with mild lissencephaly who may experience normalized development, more adjusted to their age group, gender and school level..



Yet No Comments