
The pleural fluid is a plasma ultrafiltrate that acts as a biological lubricant of the pleural cavity, helping the movement of the lungs during respiration (inhalation and exhalation).
The amount of pleural fluid is very small, approximately each hemithorax houses 5 to 15 ml. It is located inside the pleural cavity, which comprises the space between the outside of the lungs and the thoracic cavity. The membrane that delimits this area is called the pleura.
In different pathologies an increase in pleural fluid can occur and an effusion may occur. This increase can occur due to the production of transudates or exudates.
Establishing the difference between exudate and transudate is essential to reach the diagnosis. Cytochemical analysis determines whether the accumulated fluid is a transudate or exudate. For this, the Light criteria are followed, determined mainly by the pH value, total proteins, LDH and glucose..
However, today other analytes have been added that help to differentiate the transudate from the exudate, increasing the precision..
The most frequent pathologies that produce transudations are: congestive heart failure, neoplasms, decompensated liver cirrhosis, chronic kidney failure or pulmonary embolism, among others.
It can also occur in other less common causes, such as: constrictive pericarditis, Dressler syndrome, nephrotic syndrome, hypothyroidism, peritoneal dialysis, Meigs syndrome, among other causes. While, infectious, neoplastic, inflammatory pathologies, among others, can cause the formation of exudates.
The cytochemical, smear microscopy, Gram and culture are laboratory tests that guide towards the origin of the pleural effusion.
Article index
Pleural fluid is necessary for the proper functioning and homeostasis of the respiratory system. Keeps the pleura lubricated and, in this way, the lungs can easily expand and retract, without friction between the parietal and visceral pleura.
The pleura is a membrane that has two leaves, the parietal (attached to the thoracic cavity) and the visceral (attached to the lungs).
Both are irrigated by vessels of the systemic circulation, however, the venous return is different, since in the case of the parietal sheet, the capillaries drain through the vena cava, while the visceral sheet returns through the pulmonary veins..
Pleural fluid is an ultrafiltrate of the blood, which flows through the capillaries at a rate of 0.5 ml / hour into the pleural space. The parietal sheet is crucial in the absorption of the pleural filtrate and the cells found within the pleural cavity.
If an imbalance occurs in the circulation (increased production or incorrect reabsorption), the liquid accumulates and can generate a spill. Among the causes that can cause a pleural effusion are:
- The formation of transudates (hydrothorax) is formed from the pulmonary capillaries: by an increase in hydrostatic pressure and capillary permeability, by a decrease in oncotic pressure and by an increase in the negative pressure of the pleural space.
- Also due to altered lymphatic flow or invasion of ascitic fluid into the pleural cavity.
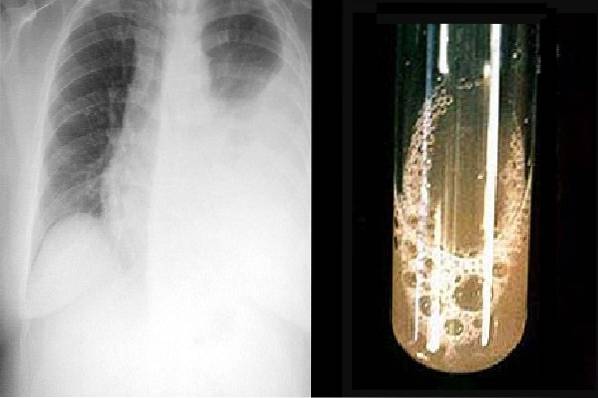
Radiographic studies may reveal the existence of a pleural effusion. In minimal effusions, other tests are sometimes necessary, such as chest CT scan or chest ultrasound..
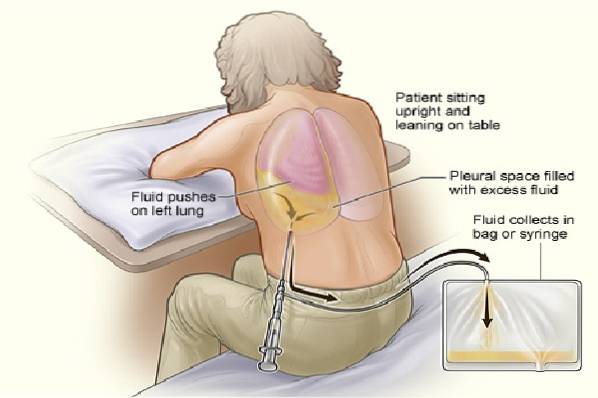
The extraction of pleural fluid for analysis is indicated in patients who have suffered a pleural fluid effusion. The cytochemical and culture of the pleural fluid can help determine the cause.
Pleural effusion is a very dangerous clinical complication, the main symptoms being dyspnea, pleuritic pain or a dry cough..
Pleural effusion can be primary or secondary. Primary when there is a pathology of the pleura and secondary when it occurs due to extrapleural involvement.
Pleural fluid is removed through a procedure called thoracentesis. This must be done by a doctor. The liquid is collected in different tubes according to the analyzes.
Determining the cause of the pleural effusion is crucial to establishing effective treatment.
For the cytochemical analysis, the sample must be collected in sterile tubes with heparin anticoagulant for the biochemical study and with EDTA for the cell count. Anticoagulants should be used because this fluid tends to clot..
The cytochemical study includes: physical study, biochemical study and cytological or cellular study.
Determination of pH, density, color, appearance.
Glucose, total protein, lactate dehydrogenase (LDH) enzyme.
Sometimes the doctor may request additional tests, especially when specific pathologies are suspected: Examples:
-Pleural effusions due to tuberculosis: determination of adenosine deaminase (ADA), lysozyme and interferon gamma.
-Chylothorax: the triglyceride value is very useful, in general the pleural fluid is milky, although there are exceptions.
-Pseudochylothorax: determination of cholesterol.
-Pancreatitis and pancreatic pseudocyst: determination of amylase.
-Urinothorax: determination of creatinine.
-Lupus pleurisy: antinuclear antibodies (ANA).
-Rheumatoid arthritis pleural effusions: Complement (C4), rheumatoid factor.
-Mesotheliomas: Pleural Mesothelin.
Red blood cell and leukocyte count, leukocyte formula.
Pleural fluid for microbiological analysis should be collected in a sterile tube..
To perform the Gram, the pleural fluid is centrifuged and a smear is made with the sediment of the fluid. It is stained with the Gram stain and observed under a microscope..
Pleural fluid is naturally sterile, therefore any organisms observed are of clinical importance. It must be accompanied by a culture.
With the sediment of the liquid, a smear is made for BK (Ziehl Neelsen stain to search for Koch's bacillus, Mycobacterium tuberculosis). However, this study has low sensitivity.
The sediment of the pleural fluid is seeded in nutritious culture media: blood agar and chocolate agar. A Sabouraud agar can also be included for the study of fungi and by means of Löwenstein-Jensen in case of suspicion of Mycobacterium tuberculosis. The latter usually requires a previous step of decontamination of the sample with NaOH 4%.
However, if bacteria are not observed on the Gram, it is not necessary to decontaminate the sample. In this case, the sediment is sown directly on the Löwenstein-Jensen medium..
Study of anaerobic bacteria can also be included, especially in pleural fluids that present a foul odor..
Biopsy is necessary in certain neoplasms. Can be tested through pap smear of pleural fluid.
Sometimes a thoracoscopy is required. This moderately invasive procedure is relevant when other non-neoplastic etiologies have been ruled out. It is contraindicated when there is a risk of bleeding. It consists of the induction of an artificial pneumothorax for curative or diagnostic purposes.
Procedure used to explore the airways, using a bronchoscope.
There may be pleural effusions that have normal values, that is, there is an accumulation of fluid, but there are no major changes in its composition and appearance. This type of liquid corresponds to a transudate. They are usually more benign.
pH: similar to plasma pH (7.60-7.66). It must be measured in a blood gas equipment.
Density: < 1,015.
Appearance: Transparent.
Color: Light yellow (watery).
Odor: odorless.
Total protein (PT): 1 - 2.4 g / dl.
LDH: < de 50% del valor plasmático.
Glucose: similar to plasma.
Cells: count < de 5000 cel/mm3
Formula: predominance of lymphocytes, macrophages and mesothelial cells.
Red blood cells: they must not exist or they are very scarce.
Mesothelial cells: their count is not clinically important.
Neoplastic cells: Absent.
ADA: < de 45 U/L.
Pleural fluid lysozyme / plasma lysozyme ratio: < 1,2.
Gamma interferon: < 3,7 UI/ml.
Culture: negative.
Gram: No microorganisms observed.
BK: Acid-fast bacilli are not observed ...
Other types of pleural effusions not only present with an exacerbation of the fluid, but there are also important physical, biochemical and cytological changes. These correspond to the exudates.
Transudate: 7.45-7.55.
Exudates: 7.30-7.45.
It can reach lower figures (< 7,0-7,20) en derrames de origen paraneumónico, tuberculoso, neoplásicos, entre otras causas.
> 1,015.
Purulent and thick (empyema).
Milky and watery (chylothorax and pseudochylothorax).
Yellowish (serous).
Orange when it contains moderate red blood cells (serohematic).
Reddish or bloody when it contains abundant red blood cells (hemothorax).
Milky whitish (chylothorax).
In urinothorax, the pleural fluid has a characteristic urine odor. While it may have a foul or putrid odor in infections caused by anaerobic microorganisms.
Total proteins: Pleural fluid PT / plasma PT ratio> 0.5 or total pleural fluid proteins> 3 g / dl.
LDH: > 2/3 of the upper limit normal value of plasma (> 200 IU / ml) or ratio pleural fluid LDH / plasma LDH> 0.6
LDH values> 1000 IU / ml are indicative of pleural effusion due to tuberculosis or neoplasms.
Glucose: decreased values with respect to plasma. It can reach values close to zero in case of empyemas, tuberculosis, etc..
Counting:> to 5000 cel / mm3 (although some authors consider it pathological above 1000 cells / mm3). Values> 10,000 mm3 suggest parapneumonic pleural effusion.
Red blood cells: Moderate to abundant red blood cells. In hemothorax, the count can reach 100,000 cells / mm3, (hematocrit> 50% of blood).
Leukocyte formula: cellular predominance can aid differential diagnosis, especially in exudates.
Neutrophil-predominant pleural effusions: increased in inflammatory pleural effusions. Example in pneumonia, acute tuberculosis, pancreatitis, pulmonary embolism and some neoplasms.
Lymphocyte-predominant pleural effusions: it is generally elevated in the case of pleural effusions due to chronic tuberculosis, or due to malignancy (exudates), although there are usually other causes (chylothorax, lung transplant rejection, pulmonary embolism, sarcoidosis, among others). The lymphocyte count has no diagnostic value in the case of transudates.
Pleural effusions with eosinophilia (> 10%): Fluids with a high number of eosinophils rule out malignant or neoplastic etiology. It is frequent in parasitic or fungal infections, in pleural effusions due to trauma, in spontaneous pneumothorax, cirrhosis, sarcoidosis, among others..
According to the clinical suspicion, the doctor may request additional studies or analytes, including:
ADA:> 45 U / L (tuberculosis).
Pleural fluid lysozyme / plasma lysozyme ratio: > 1.2 (tuberculosis).
Gamma interferon: > 3.7 IU / ml in tuberculosis
Cholesterol: trasudados < de 60 mg/dl, exudados > 60 mg / dl (pseudochylothorax).
Triglycerides: > 110 mg / dl or above plasma level (chylothorax).
Amylase: > than the plasma value, (pancreatitis, pancreatic pseudocysts, esophageal rupture.
Pleural fluid creatinine / plasma creatinine ratio: > 1 (urinothorax).
Creatinine: < al nivel sérico (insuficiencia renal crónica).
ANA: titers> 1: 160 or above the plasma value, (lupus pleurisy).
Rheumatoid factor: titers above 1: 320 or higher than the plasma value (rheumatoid pleurisy).
C-Reactive Protein (CRP): CRP ratio of pleural fluid / CRP of serum> 0.41. If the CRP value exceeds 100 mg / L, the effusion is considered to have a complicated prognosis..
Pleural mesothelin: > 20 nM (Mesotheliomas).
Natriuretic peptides: present (heart failure).
Complement C3 and C4: in exudates they are low, especially in pleural effusion due to tuberculosis or malignant diseases. While C4 figures < 0,04 g/dl, sugieren derrame por artritis reumatoidea.
Ferritin: values> 805 µ / L exudate but> 3000 µ / L (indicates malignant pleural effusion).
Pleural fluid ferritin / serum ferritin ratio: > 1.5-2.0 (exudate).
In case of infectious pleural effusions:
Culture: positive. The most commonly isolated microorganisms are: Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Escherichia coli Y Pseudomonas aeruginosa.
Gram: Gram-positive or Gram-negative cocci, bacilli, or coccobacilli may be seen.
BK: acid-fast bacilli (tuberculosis) may be seen.
Neoplastic cells: it is studied through cytology of pleural fluid. However, sometimes it is necessary to perform analysis by immunohistochemical techniques and flow cytometry. These techniques make it possible to distinguish cases of metastatic adenocarcinoma, mesotheliomas, and lymphomas..


Yet No Comments