The Brandt-Andrews maneuver is an obstetric technique that is applied to extract the placenta and umbilical cord in the last stage of labor, once the mother expels the child.
The procedure is based on the doctor cutting the umbilical cord that connects the child with the placenta. Later, the stage of placental detachment and expulsion begins, which is known as delivery.
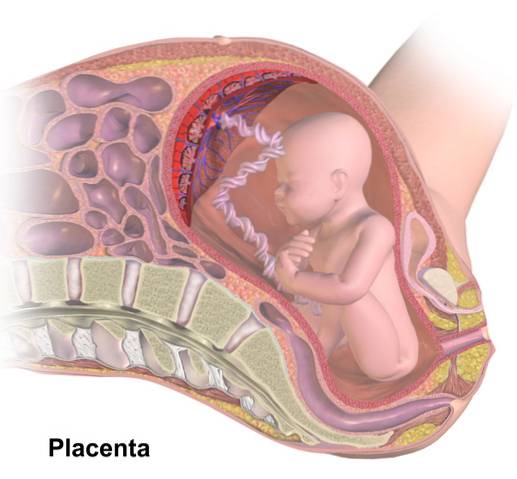
The placenta is an organ that originates from the cells of gestation and is responsible for maintaining fetal vitality through the exchange of nutrients, oxygen and hormones that it receives from the maternal circulation..
Once the expulsion of the child occurs, the placenta begins a process of natural detachment that can last up to 30 minutes.
The technique proposed by the North American obstetricians Murray Brandt and Charles Andrews consists of facilitating the placental exit by applying firm but subtle pressure from the umbilical cord, with one hand, while holding the uterine fundus fixed with the other. In this way the doctor can evaluate the bleeding, the consistency of the uterus and the integrity of the placenta, to avoid later complications.
Article index
Dr. Murray Brandt was a New York obstetrician who dedicated his professional life to studying the mechanism of childbirth. He was one of the first professionals to clarify that the separation and expulsion of the placenta were two different processes.
In 1933 he published his work Mechanism and Management of the Third Stage of Labor, in which he described a maneuver to facilitate placental outflow and avoid eversion of the uterus, a complication that was frequently observed with the technique used previously.
Later, in 1940, Norfolk, Virginia obstetrician Charles Andrews introduced a modification to the Brandt maneuver..
Around 1963 it was decided that both techniques were equally important and complementary, so the eponymous Brandt-Andrews began to be used to refer to the union of both descriptions of the procedure.
Murray Brandt described in 1933 his technique to facilitate placental expulsion, which he developed through a study involving 30 patients in the period of delivery that comes after the expulsion of the fetus, called delivery.
In each case, they waited between 5 and 10 minutes for the baby to come out and proceeded to place a surgical clamp on the umbilical cord that protruded through the vulva..
With one hand, the fundus of the uterus should be located, which is contracted with a hard consistency. Meanwhile, the clamp and umbilical cord are held with the other hand until it is felt to be easy to pull it out. This means that the placenta has detached and can now be manually helped to expel it, without danger..
While the umbilical cord is found, the uterus is held firmly in place with the other hand, seeking to elevate it.
In 1940 Charles Andrews added a modification to the original procedure described by Murray Brandt. First, the descent of the umbilical cord is expected, indicating placental abruption.
Subsequently, a firm and slow traction is made with the hand that manipulates the cord while, with the other hand, the uterus is gently massaged to stimulate contraction and facilitate placental abruption..
Both techniques emphasize holding the uterus firmly in position and, if possible, pushing it vertically upward..
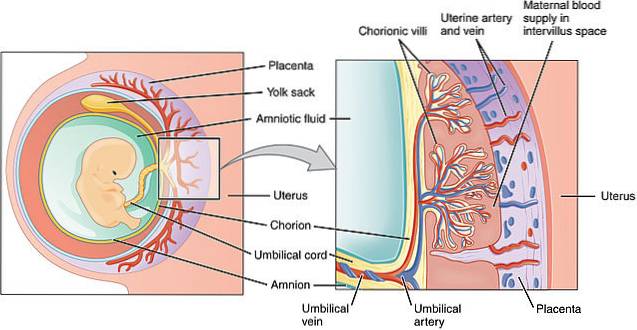
The placenta is a specialized and complex organ that forms around the 4ta week of gestation and that guarantees fetal vitality within the uterus.
It is attached to the uterus and has a rich network of blood vessels which connects with the maternal circulation. Through this vascular matrix it performs functions of exchange of gases, nutrients, hormones and also acts as a barrier against some harmful particles.
After birth and the interruption of circulation with the separation of the umbilical cord, the placenta begins a process of detachment and expulsion through the vaginal canal. This moment represents the third stage of labor and is known as delivery.
Delivery lasts about 30 minutes, however, some specialists agree that maneuvers should begin to facilitate the process in case there is no natural expulsion 10 minutes after birth..
When a natural delivery does not occur, the pertinent maneuvers are carried out to facilitate placental detachment and expulsion. This is known as active management of the third stage of labor, being the Brandt-Andrews technique the most used maneuver.
The Credé maneuver was the one carried out since 1853. It consisted of making abdominal pressure near the symphysis pubis while pulling the umbilical cord with force, but it brought serious complications in many cases..
The Brandt-Andrews maneuver avoids postpartum complications, when done correctly. By stimulating the uterus in such a way that it continues to contract, it is achieved that it does not enter a passive state, in which detachment is not possible. Uterine contractions at this stage also prevent massive bleeding that can be fatal.
The cord traction described according to the Brandt-Andrews maneuver, securing the uterus, prevents uterine inversion. That is, the inner part of the uterus protrudes through the vagina. This complication was frequent with the technique described by Credé.
When the placenta remains inside the uterus for more than 30 minutes it is considered a complication of childbirth known as placental retention. This can lead to infection of the uterine cavity.
Another complication that can occur due to poor technique on the part of the doctor is the detachment of the umbilical cord, which causes bleeding and placental retention..
This phenomenon is due to exaggerated traction on the umbilical cord in a placenta that has not completely detached from the uterine fundus..
Management in these cases is surgical and emergency, since it represents a danger to the life of the patient..



Yet No Comments