
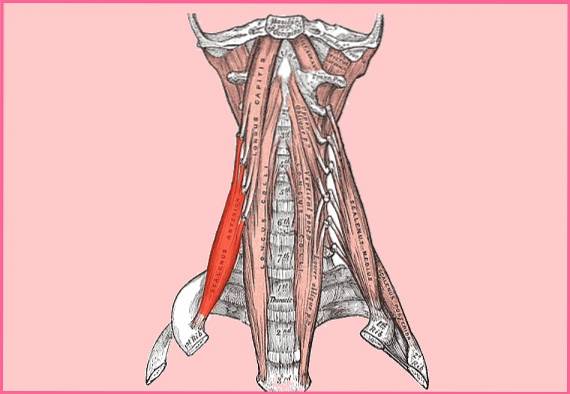
The anterior scalene muscle It is an anatomical structure that is located at the level of the neck, in the deep anterolateral region. Its fibers descend obliquely from their areas of origin at the level of the cervical vertebrae C3 to C6, to the place of insertion at the level of the first rib.
It is a deep, even, irregularly shaped, cone-like muscle. Laterally it is covered by the trapezius muscle and the levator scapulae. It is found close to its counterparts, the middle and posterior scalene muscles..
Between one and the other there are spaces called interscalene hiatuses or gorge of the scalenic ones. It should be noted that the most relevant of these spaces is the one located between the anterior scalene muscle and the middle scalene, frequently called the interscalene triangle, with the base of the triangle being the first rib.
Its importance lies in the fact that the subclavian artery passes through it, as does the brachial plexus that runs above the subclavian artery. While the subclavian vein passes in front of the anterior scalene (outside the triangle).
Knowing the anatomical relationships is very important, as it helps to understand certain clinical manifestations that can occur when these muscles undergo spasms..
Spasms can generate direct or indirect compression of the aforementioned adjacent anatomical structures, especially on the brachial plexus and secondarily on the subclavian artery..
Article index
The anterior scalene muscle originates from the vertebrae that are at the level of the neck, specifically it arises from the anterior tubercles of the transverse processes of the third cervical vertebra to the sixth cervical vertebra (C3-C6).
The muscle descends from its points of origin, passes below the clavicle and then inserts at the level of the anterior arch of the first rib. The place where the muscle is attached to the rib is called the Lisfranc tuber or the anterior scalene tuber..
An interesting fact is that Lisfranc's tubercle is located behind the groove of the subclavian vein and in front of the groove of the subclavian artery, all arranged in the first rib. That is why the anterior scalene muscle has a close relationship with these anatomical structures.
The anterior scalene muscle receives innervation from the anterior branch of the spinal nerve C4, C5, C6 and C7 (C4-C7), which means that it receives innervation from both the cervical plexus and the brachial plexus.
This muscle is supplied by the ascending cervical and inferior thyroid arteries..
Its insertion in the first rib is not by chance, this serves to raise the first rib, that is why it is considered an accessory muscle of respiration, since it participates secondarily in the inspiratory movement.
In addition, it also executes the rotation movement of the neck, towards the opposite side of the muscle in action. That is, the anterior scalene muscle on the right side rotates the head to the left side and vice versa..
On the other hand, it also participates in the flexion of the neck laterally towards the same side of the muscle in action (ipsilateral) and in the anterior flexion of the neck.
It should be noted that these movements described here are reinforced by the middle and posterior scalene muscles, that is, they act synergistically with their counterparts..
Many back, shoulder and arm pains can be originated from a trigger point at the level of the anterior scalene muscle and to a lesser extent they can also cause headaches, chest pain and the medial edge of the scapula.
Unfortunately, other causes are always sought, while the scalene muscle is ignored.
It is very common for the pain to radiate down the arm, affecting the biceps and triceps. Then the elbow jumps, to reappear again on the radial side of the forearm. Pain can continue to the thumb and index finger.
When the pain radiates to the chest on the left side, it can be mistaken for angina pectoris.
Rajanigandha et al. In 2008, described a case of the presence of an accessory or aberrant scalene muscle. The find was found in the corpse of a 56-year-old woman..
They observed the presence of an accessory muscle fascicle measuring 6.2 cm in length and 1.3 cm in width..
This accessory muscle arose from the middle of the anterior surface of the middle scalene muscle. The presence of this aberrant muscle undoubtedly represented a predisposing factor for neurovascular compression for this patient..
Knowing these types of anatomical variations is of crucial importance for surgeons.
The term Thoracic Outlet Syndrome (TOS) was created to describe cases with compression of the subclavian vein or artery or of the brachial plexus, in which anterior scalene syndrome is included..
Compression can occur at the level of three emblematic anatomical areas, which are: the interscalene triangle (it is the one that concerns us), the costoclavicular space and the subcoracoid space.
The origin of compression can be very varied, but it is mainly associated with anatomical variations of certain structures, such as: presence of aberrant or supernumerary muscles, tendons or ligaments or presence of normal anatomical structures with an unusual trajectory.
They may also affect other factors, such as anterior fractures or the presence of fibrosis, spasms, or shortening of the anterior or median scalene muscle..
These causes can generate a significant decrease in the lumen of the interscalene triangle, this causes the subclavian artery and / or the brachial plexus or both to be compressed..
Vascular compression of both the artery and the subclavian vein can cause arterial or venous thrombosis.
Compression at the level of the subclavian vein is called Paget-Schroetter syndrome. This syndrome is characterized by edema and venous congestion of the upper limb.
Whereas, compression of the subclavian artery causes digital pallor with or without subsequent cyanosis, Raynaud's phenomenon, or hypothermia, among others..
In nerve compression, the symptoms usually guide the diagnosis. It is usually characterized by mild, moderate and severe paresthesias, as well as muscle atrophy, especially of the muscles of the hand.
The Adson test can be used to detect neurovascular compression. Catheterization is also useful as a diagnostic method in case of vascular compression.
The Adson maneuver or test is a test that evaluates whether or not there is neurovascular compression at the level of the interscalene triangle. For the test it is necessary for the patient to sit on a stretcher, while the specialist stands behind him..
The test consists of placing the patient's arm in 90 ° abduction concomitantly with a maximum external rotation of the shoulder.
Then, with one hand in a guitar playing position, the wrist is grasped to palpate the pulse of the radial artery and with the other the head is rotated contralaterally, with the idea of stretching the scalene muscles. At this time the patient must inspire strongly.
If during this maneuver the radial pulse disappears or there is paresthesia (tingling sensation) or paresis (weakness) in the arm, the test is considered positive for thoracic outlet syndrome.
Treatment of compression of these structures is almost always surgical. One of the decompression methodologies used at the medical level is the transaxillary technique of extraction of the first rib or also the anterior scalenotomy.
The anterior scalene is a fairly tonic muscle and this causes them to be over-tensioned at times.
To massage these muscles, friction must be done in a transverse way to how the muscle fibers go. The massage is given mainly towards the insertion site, that is, at the level of the first rib. This site is the most vulnerable to suffer from fibrous tracts.
Another way to massage the scalene muscles is to place the fingers just in the groove that is made behind the clavicle, especially when we lean the head forward..
With great care we can insert our fingers there and gently massage said area. This place is very delicate because there are many blood vessels and nerves. It is important to combine the massages with breathing exercises, to further relax the anterior scalene.



Yet No Comments