
The subscapularis muscle It is part of the rotator cuff. Therefore, it provides stability to the shoulder joint (glenohumeral), together with the supraspinatus, infraspinatus and teres minor muscles..
While the supraspinatus, infraspinatus, and teres minor muscles hold the glenohumeral joint superiorly and posteriorly, the subscapularis does so anteriorly..
It should be noted that stabilization of the shoulder on the anterior surface is not only a function of the subscapularis muscle, but also other structures such as the coracobrachial ligament, the anterior capsule itself and the ligaments of the glenohumeral joint, both superior, middle and inferior..
The participation of the subscapularis muscle in stabilizing the shoulder is limited to generating an eccentric tension, which regulates the anterior translational movement (slide). This function is possible thanks to the strategic points of origin and insertion.
Other functions of the subscapularis muscle, apart from stabilizing the glenohumeral joint, is to assist in internal rotation of the shoulder. Also, depending on the position of the joint, it participates in the movement of abduction, flexion, extension and depression..
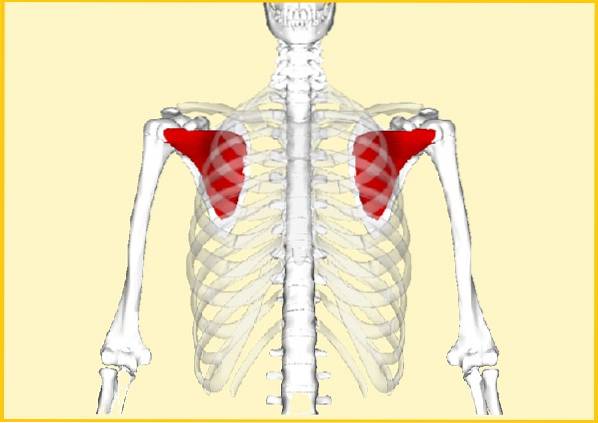
The subscapularis muscle originates in the anterior part of the shoulder blade or scapula, specifically in the fossa that bears the same name "subscapularis" and extends to the head of the humerus, inserting in greater proportion in the lesser tubercle, while a small portion does in the greater tuber.
The subscapularis muscle is the strongest of the 4 mentioned, and for this reason subscapularis tendonitis is difficult to diagnose, giving positive signs only when it is seriously injured.
Article index
The muscle has a triangular shape, thick edges and a broad body.
The subscapularis muscle is located in the anterior part of the scapula, originating in the subscapular fossa, specifically in the costal area. The body or belly of the muscle covers the subscapular fossa. The muscle passes over the back muscles.
The muscle attaches to the anterior portion of the humeral head, the area of which is called the lesser tubercle or troquin..
The subscapularis muscle is innervated by two nerves and because of this it is divided into two sections, fibers upper-subscapularis Y lower-subscapularis, that is, superior and inferior fibers of the subscapularis.
The first portion is innervated by the superior subscapular nerve (C5-C6) and the second by the inferior subscapular nerve (C5-C6). Both nerves come from the brachial plexus.
This muscle has a blood supply in charge of the transverse cervical artery and the subscapular artery mainly. However, a work published by Naidoo et al. showed that there are anatomical variations between one individual and another. To do this, they studied 100 corpses and observed the following:
In 96% of cases, the subscapular muscle was supplied by the subscapular artery, in 39% by the thoracodorsal artery (branch of the internal subscapular artery), 36% by the suprascapular artery, in 14% by the lateral thoracic artery and in 9 % by the circumflex scapular artery (branch of the subscapular artery).
It is a co-receptor of the glenohumeral joint, that is, it contributes, together with other muscles, to keeping the head of the humerus stable within the glenoid cavity despite movements. The support function is fulfilled from the anterior face of the glenohumeral joint.
On the other hand, one of its main functions is to collaborate with the internal rotation movement of the shoulder, a function that it exercises together with other nearby muscles, such as: sternal fibers of the pectoralis major, teres major and latissimus dorsi.
However, internal rotation of the shoulder is not the only function it exercises, since depending on the position adopted by the humeral head in relation to the scapula, the subscapularis muscle can collaborate as: abductor, extensor, flexor and depressor.
It is even believed that it can help in the external rotation movement in some positions, due to the joint insertion that it has with the supraspinatus and infraspinatus muscles..
Some authors believe that the subscapularis muscle in the 90 ° abduction position at the level of the shoulder blade exerts a force equivalent to that of the infraspinatus and 2.5 times greater than that of the supraspinatus..
On the other hand, the function of the subscapularis muscle can be divided according to the area, that is, the upper part of the muscle fulfills one function and the lower part another..
In this sense, Ackland et al cited in Collard et al., they ensure that the upper part of the subscapularis muscle is the one that most favors the internal rotation movement; obtaining a maximum point at 30 ° of flexion and abduction in the joint.
While, the lower part is specifically responsible for stabilizing the posterior joint, counteracting the anterior translation.
One of the most common disorders that occur in the muscles that make up the rotator cuff is injury to the subscapularis muscle. The injury can be caused by contraction of the muscle (shortening) or overstretching (lengthening).
If the muscle is tense, trigger points may appear, which cause pain, which is easily correctable with rest and massage..
However, this may be the beginning of other more complicated situations, which can generate chronic pain.
The location of the muscle gives it a peculiar situation, since of the four muscles, the subscapularis is the only one that is positioned in the anterior part of the scapula. Therefore, its function as a co-receptor of the anterior aspect of the glenohumeral joint cannot be supplied by the rest of the muscles..
In any case, other nearby muscles such as the pectoralis major, the round and the latissimus dorsi can dominate the internal rotation movement, but these are not co-receptors of the glenohumeral joint.
In this sense, if the muscle becomes weak or lengthens, the reinforcement of the glenohumeral joint in its anterior part will be threatened, leaving only at the expense of the joint capsule and the coracobrachial and glenohumeral ligaments, which are less strong..
This situation causes an exaggerated anterosuperior gliding, a symptom that precedes the subacromial syndrome..
In external rotation, the normal thing that should happen is that the external rotator muscles contract, while the subscapularis is stretched. The found forces generated on both sides of the joint are what provide stability to the humeral head in the glenoid cavity..
However, the subscapularis muscle can become weak or elongated as a result of stiffness or shortening of the external rotator muscles..
This causes a limitation in internal rotation, since the effort made by the subscapularis muscle during external rotation under this circumstance, causes it to overstretch and weaken over time..
Other factors that can injure the muscle are found in: the adoption of bad postures, the excessive use of the shoulder joint, sudden movements without warming up, static positions for a long time or previous degenerative diseases such as arthritis, among others. Several causes can coexist at the same time.
Most tears occur at the junction of the tendon with the bone (tenoperiosteal junction). This involvement causes pain in the back of the arm and occasionally the pain can radiate to the wrist..
Likewise, a tear of the subscapularis muscle at the level of the muscle belly produces pain at the level of the scapula, but this is not frequent..
The tear is usually healed naturally with scar tissue, but it is easily ruptured with moderate effort. If this situation is repetitive, the muscle weakens and becomes painful..
Depending on the cause, the symptoms may appear gradually or suddenly. In cases of slow progression, the patient mainly complains of pain when raising the arm above the shoulder, whatever the activity performed.
In acute cases, the problem occurs after a sudden movement, producing strong discomfort with simple maneuvers, such as: opening a door or unscrewing a cover.
If the problem is not corrected, it can cause a frozen shoulder (without movement) or osteoarthritis problems..
Subscapularis injury can also present in conjunction with a shoulder joint dislocation. In this case the pain can last for months.
The patient is asked to perform a resisted rotational movement and, if there is pain, it means that the subscapularis muscle is affected.
To do this, the arm is positioned behind the patient's back. The elbow should be flexed 90 °. Then it is tried to resist the internal rotation movement and it is observed if there is pain.
Although it is very difficult to palpate the muscle, some massages can be done that can relieve pain.
There are two self-massage techniques, the first called pressure-movement, which consists of touching the muscle and exploring the areas of pain, while performing the internal and external rotation of the shoulder joint repeatedly..
While the second is called the thumb technique. The thumb is placed in an immediate area to the point of pain to begin to massage it repeatedly.
It is also very useful to perform stretching exercises.
It is also known as rotator cuff tendonitis or impingement. It is a very common affection in young patients.
It develops in three stages:
1) Edema and inflammation of the affected muscle.
2) Compression of the rotator cuff due to fibrosis and thickening of the subacromyodeltoid serous bag.
3) Partial or total tear of the muscles that make up the rotator cuff, the subscapularis muscle may be involved.



Yet No Comments