
The trigeminal neuralgia (NT) is a painful, unilateral facial pathology that is described as a brief episode of electric shock or burning sensation. Specifically, the pathologies that cause facial or craniofacial pain constitute a series of diseases that include a large number of medical conditions: facial neuralgia, symptomatic facial pain, neurological signs, trigeminal autonomic headaches, and facial pain without neurological symptoms or signs..
Thus, trigeminal neuralgia is considered one of the most severe and intense facial pain symptoms. Although its annual incidence varies, it usually occurs in people over 50 years of age and, in addition, substantially alters the quality of life of those affected.
Regarding the etiological cause of trigeminal neuralgia, it is normally associated with an understanding or mechanical tension of the trigeminal nerve as a result of vascular factors: abnormalities in blood vessels, arterial hypertension or dyslipidemia, among others..
The diagnostic evaluation of this pathology is usually carried out based on a detailed study of the characteristics of pain and various imaging studies, which allow detecting the presence of neurological alterations..
Regarding the treatment of trigeminal neuralgia, initial interventions focus on drug prescription. However, in severe cases, surgical interventions or percutaneous techniques may be chosen..
Article index
Trigeminal neuralgia, also known as “tic pain”, is a pathology that causes neuropathic pain, that is, pain associated with various nerve abnormalities or injuries.
The clinical definition of this pathology dates back to the seventeenth century. Since ancient times it has been referred to as " the most intense pain that man can suffer”. Furthermore, in the most recent clinical reports, trigeminal neuralgia is still classified as “one of the worst causes of pain suffering".
The pain derived from this pathology is characterized by different episodes of stabbing, burning pain, or a sensation of cramp and electric shock in the craniofacial areas innervated by the trigeminal nerve..
In addition, it usually appears when eating, brushing teeth, touching the face, etc. , making it mentally and physically disabling.
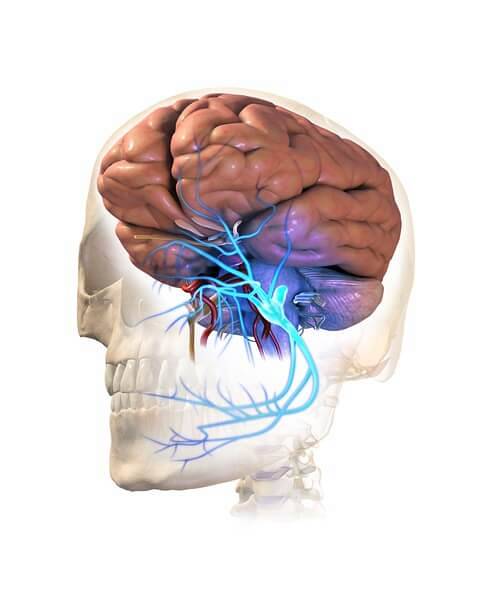
The trigeminal nerve or cranial nerve V, is a nervous structure that has a mixed function: motor and sensory. Thus, its essential function is to control the muscles and facial sensitivity:
The sensitive branches of the trigeminal nerve are responsible for conducting the nerve impulses related to tactile sensations (external stimulation, proprioception and pain) of the anterior areas of the tongue, the teeth, the dura mater (outermost meningeal layer), the oral mucosa and the paranasal sinuses (cavities located in the maxillary, ethmoid, sphenoid and frontal bone areas).
The motor branches of the trigeminal nerve supply mainly the mandibular areas: masticatory muscles (temporal, mastero-pterygoid) and, in addition, the tensor tympani, mylohyoid and dysgastric muscles.
This nervous structure, in turn, is divided into 3 fundamental branches:
Due to these characteristics, when the trigeminal nerve is damaged or injured in one or more of its branches, this pathology is associated with a significant decrease in quality of life and ability to work. It is also common for many affected people to develop depressive syndromes.
Trigeminal neuralgia is a medical condition that usually occurs chronically.
Although there are few statistical data on this pathology, it has been possible to identify that it presents an approximate incidence of 12 cases per 100,000 people per year.
It is estimated that in the United States about 140,000 people can live with this pathology.
It has been observed that, depending on sex, it affects mostly women and that, in addition, it is more prevalent in the population over 50 years of age.
However, trigeminal neuralgia is a pathological condition that can develop any person, man or woman and at any stage of maturation..
The essential clinical feature of trigeminal neuralgia is the presence of episodes of facial pain characterized by:
Although the presentation of these episodes can be variable among the affected people, the intensity of pain is often defined as unbearable, keeping the individual immobile..
Regarding the most affected areas, the pain typically appears on the cheek or in the jaw and occasionally, in the areas surrounding the nose and eyes, although this situation will fundamentally depend on the affected nerves..
In addition, this pathology can also be classified into two different types, depending on its clinical course:
This pathology is classified in two differential forms depending on its cause:
Although the factors that can lead to the development of this pathology are diverse, all will affect the trigeminal nerve, causing injuries and / or mechanical compression.
Among the most common causes of trigeminal neuralgia are:
The diagnostic evaluation that is usually used in pathologies related to facial pain is mainly focused on clinical analysis, paying special attention to details..
The essential objective is, therefore, to carry out an anamnesis to recognize the clinical and evolutionary profile of pain:
In addition, this is usually accompanied by a physical examination that confirms some data such as the anatomical distribution or the triggers..
On the other hand, the use of complementary laboratory tests, such as magnetic resonance imaging, is also frequent. This test allows us to identify the presence or absence of a nerve involvement in the branches of the trigeminal nerve..
Similarly, the identification of the possible etiological medical cause is another essential point, since it will allow the design of an effective and individualized therapy..
Various therapeutic interventions have been described in the medical literature and in professional practice that are effective both in the treatment of the signs and symptoms of trigeminal neuralgia and in the control of etiological medical conditions..
The initial treatment of facial pain usually includes various drugs: analgesics, anticonvulsants or muscle relaxants. In some patients, pain can be treated through opioids such as methadone or antidepressants, used to treat other types of neuropathic pain.
Although this approach is usually effective in the initial episodes, many patients have adverse reactions such as myelosuppression, drowsiness, ataxia, or fatigue..
In the most severe cases, there are other options such as surgery. However, its use will depend fundamentally on the characteristics of the patient and the identification of the cause of trigeminal neuralgia..
Some interventions include:
Through this procedure, a high dose of radiation is applied to a particular area of the trigeminal nerve. It is used to produce a lesion in it that allows interrupting the transmission of pain signals to the brain.
Through the insertion of a needle in areas that allow to reach the trigeminal nerve, especially through the foramen ovale in the cheek, the fibers are damaged or destroyed to prevent the conduction of pain.
Through a craniotomy and the placement of a pad between the blood vessels that compress the trigeminal nerve, it is possible to relieve neurovascular pressure and consequently, pain symptoms.
Although it is the most effective, they present significant risks: facial weakness, paresthesia, diplopia, loss of hearing, cerebrovascular accident, among others..



Yet No Comments