
The opsomenorrhea It is a disorder of the menstrual cycle of women that consists of the presentation of prolonged cycles with intervals greater than 35 days. Normally, a menstrual cycle should last 28 days, with a variability of approximately ± 3 days.
The word "opsomenorrhea" derives from the Greek opso (too late), men (less) and rheo (flow) and specifically means: menstruation that occurs at too long intervals. An increase greater than 5 days above the maximum limit of the normal range and not greater than 90 days is defined as opsomenorrhea..
Alterations in a woman's menstrual cycles can be accompanied by ovulatory or anovulatory cycles. They usually appear as alterations in the periodicity of menstruation, the intensity of menstrual flow, the duration of bleeding, or a combination of these.
Worldwide, many schools of OB / GYN have established different nomenclatures for these disorders. In the case of opsomenorrhea, this is also known as oligomenorrhea.
The causes of opsomenorrhea are multiple and are related to some hormonal alterations such as hyperprolactinemia (increased levels of the hormone prolactin), primary hypothyroidism (decreased thyroid function) and hyperandrogenism (increased levels of androgens). ).
Opitz, in the late 1940s, was the first to coin the term "opsomenorrhea" for those menstrual disorders that occur with very long cycles, greater than 35 days..
Article index
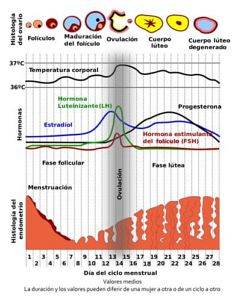
A menstrual cycle begins on the first day of menstruation and ends when the next bleeding begins. This cyclical period in the ovary occurs in three phases, the follicular phase, the ovulatory phase and the luteal phase..
Eggs are the female reproductive cells that form in the ovaries. From birth, many primordial follicles with immature eggs are found in the ovaries. Every month some of these follicles grow, but one of them develops and forms a dominant follicle.
The growth and development of the dominant follicle is what constitutes the follicular phase of the menstrual cycle. In this phase, this follicle begins to produce estrogen, a female sex hormone that is necessary for the final maturation of the follicle..
Around day 14 of the cycle, the follicle ruptures and the mature ovum is expelled into the fallopian tubes and, unless fertilization occurs, the ovum is transported from the tubes to the uterus and is eliminated through the vagina; this is the ovulatory phase of the cycle.
When the ovum is expelled, the ruptured follicle is transformed into the corpus luteum and the luteal phase of the cycle begins in which the luteal cells secrete estrogens and progesterone (hormones).
If there is no fertilization, this corpus luteum degenerates about 4 days before menstruation and is replaced by scar tissue that ends up forming what is known as corpus albicans.
From day 5 to day 14 of each cycle, the endometrium (mucosa that covers the inner surface of the uterus) proliferates and rapidly increases its thickness, which constitutes the proliferative or pre-ovulatory phase.
After ovulation and due to the effect of estrogens and progesterone, the endometrium increases its vascularity and its glands begin to secrete a transparent liquid. This initiates the luteal or secretory phase that represents the preparatory phase of the uterus for the implantation of the fertilized ovum..
As the corpus luteum degenerates, the endometrium loses its hormonal support and there is a thinning of the mucosa with the appearance of foci of necrosis (tissue death) both in the endometrium and in the vascular walls that nourish it..
The foci of necrosis produce circumscribed hemorrhages that then flow together until the endometrium is detached and menstruation occurs..
Menstrual cycles can be ovulatory or anovulatory. Three parameters characterize a menstrual cycle: periodicity, intensity, and duration.
- The periodicity refers to the date of appearance of menstruation, which normally occurs every 28 ± 3 days.
- The intensity corresponds to the amount or volume of blood eliminated during menstruation, which, on average, is 35 to 80 ml for each menstruation.
- The duration is the days that menstrual blood losses last, usually 4 ± 2 days.
Disorders of menstrual cycles can occur with ovulatory cycles or with anovulatory cycles, that is, with cycles in which there is ovulation or in which it does not occur. These disorders, in turn, can affect the parameters of the menstrual cycle.
The periodicity can be affected by shortening or lengthening the cycles. The intensity can be altered by increasing or reducing menstrual flow and the duration of menstruation. Many alterations in menstrual cycles include alterations in a combination of several parameters..
Opsomenorrhea is an alteration of the menstrual cycle that affects the periodicity of the cycle, increasing its duration to periods greater than 35 days and up to every 90 days. These alterations are frequently accompanied by anovulatory cycles and fertility problems..
In adolescence, after menarche, consultations for irregularities of the menstrual cycle are frequent. The most frequent reason for consultation is opsomenorrhea and the cause is believed to be due to a lack of development of the hypothalamic-pituitary-ovarian hormonal axis..
Opsomenorrhea is caused by a number of hormonal disorders. Almost 80% of women with PCOS also have opsomenorrhea.
Polycystic ovary syndrome is characterized by infertility, hirsutism, obesity, insulin resistance, and amenorrhea or opsomenorrhea. Generally, these patients present a continuous stimulation of the ovary by luteinizing hormone (LH), secreted by the anterior pituitary.
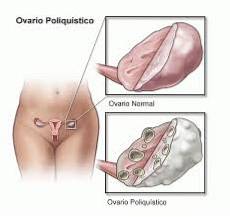
This continuous ovarian stimulation increases the production of ovarian androgens, responsible for alterations in both ovarian morphology and ovarian cycles and abnormal hair distribution in women (hirsutism).
Opsomenorrhea is also associated with hyperprolactinemia or increased blood levels of prolactin and primary hypothyroidism, that is, a decrease in thyroid function with decreased blood levels of thyroid hormones..
In adolescent opsomenorrhea, which is usually transient, treatment is conservative. It consists of observing the patient for a period of two to three years after which, in most cases, it resolves spontaneously..
In the case of PCOS, treatment depends on the woman's desire to become pregnant or not. In the first case, the treatment requires inducing ovulation. For this, the drug clomiphene is generally indicated, with or without adrenal suppression..
If the patient has polycystic ovarian syndrome and does not want to get pregnant, treatment may not be required and, in some cases, treatment is used for hirsutism, obesity, and insulin resistance..
In the case of opsomenorrhea that accompany hyperprolactinemias, treatment will be aimed at correcting the hyperprolactinemia and the same happens with primary hypothyroidism.



Yet No Comments