Plasmodium vivax it is one of the causative agents of malaria or malaria in humans. This parasite has a very wide geographic distribution and is responsible for most cases of malaria, a tropical disease, considered a major public health problem worldwide..
P. vivax, like all lhe representatives of its genus, it has a complex life cycle that includes phases that develop in two hosts. One of the hosts is an invertebrate, where the sexual phase occurs, and the other a vertebrate, where the asexual phase occurs. At least ten species out of more than 175 known species of Plasmodium they parasitize humans, four of them cause some kind of malaria.
The mosquitoes of the genus Anopheles are the vectors involved in the transmission of P. vivax. There are more than 450 species of anopheles, of which more than 50 have been identified as capable of transmitting any of the four species that cause malaria in humans. Only the female is capable of transmitting the parasite.
Studies by the World Health Organization (WHO) estimate that half of the world's population is exposed to being infected by the malaria parasite. For the year 2006, about 250 million cases and one million deaths were registered in the world. Some studies indicate that 2.85 billion people were exposed to some level of risk of transmission during 2009.
Article index
Young trophozoites are ring-shaped and can occupy up to one-third of the diameter of the erythrocyte. In it you can see a large chromatin point and the cytoplasm.
The mature trophozoite has an amoeboidal shape and is larger, occupying almost the entire erythrocyte. It has 16 merozoites inside, where chromatin and cytoplasm are appreciated in each of them.
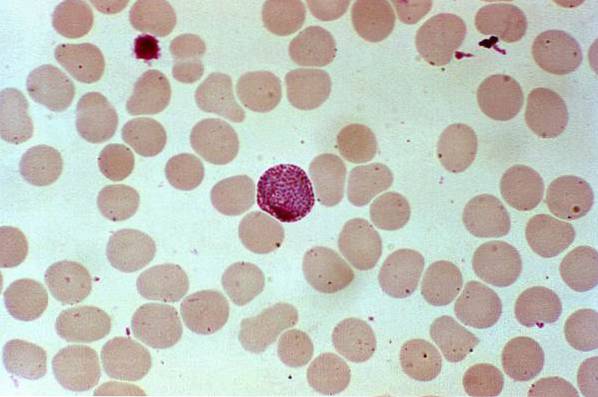
Macrogametocytes can be round or oval and have a homogeneous cytoplasm. Chromatin is small and compact, generally eccentric, with concentrated malarial pigment. While the microgametocyte is smaller, with diffuse and central chromatin, and dispersed malarial pigment.
Schizonts are large, with 12 to 24 large merozoites.
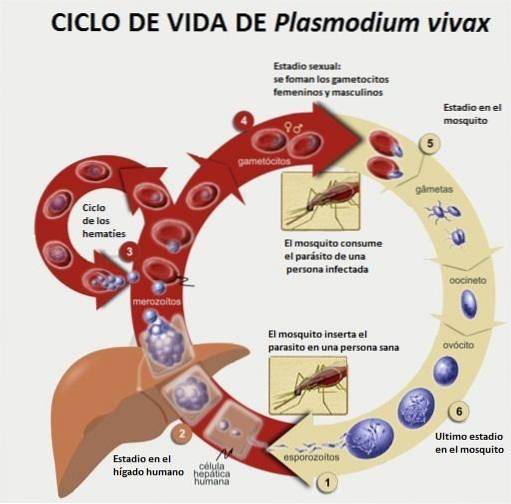
When feeding, the female mosquito of the genus Anopheles injects forms of the parasite known as sporozoites into human skin. These forms reach the liver through the bloodstream..
In liver tissue they become trophozoites, then schizonts. In successive divisions, numerous merozoites are generated, which are discharged back into the bloodstream.
Once in the bloodstream, trophozoites invade red blood cells or erythrocytes. After new divisions of the parasite, the erythrocytes break, releasing more merozoites.
Some of the cells produced develop into gametocytes, which differentiate into two types, microgametocytes and macrogametocytes. Thus, when a mosquito feeds on the infected person again, it removes the gametocytes.
The gametes fuse in the gut of the mosquito to form a zygote that transforms into a mobile form known as an ookinet and then into oocysts..
The oocysts, after multiple divisions, produce thousands of sporozoites, which migrate to the salivary glands of the insect. When the infected mosquito bites a new victim, it inoculates the infecting forms, starting a new cycle..
Malaria can be transmitted by the bite of a mosquito infested by Plasmodium, or by the transfusion of blood contaminated with that parasite.
Infection by P. vivax It can range from a parasitaemia without symptoms or a febrile picture without complications, to a serious and fatal illness.
The action of the parasite can cause chills followed by intermittent fevers, with a periodicity of 24 to 48 hours. Fever may be accompanied by headache, muscle pain, cough, diarrhea, restlessness, delirium, anemia, heavy sweating, general weakness.
These symptoms alone do not allow a precise differentiation of conditions caused by P. vivax, of those caused by others Plasmodium, or other febrile conditions.
For an accurate diagnosis, parasitological confirmation is required by microscopic examination, which can be thick blood film or peripheral blood smear, or by immunochromatographic tests.
Treatment in cases of uncomplicated malaria is based on chloroquine. Primaquine is used to prevent relapse. In cases considered complicated, Quinine is used, supplemented with the antibiotics Doxycycline or Clindamycin..
In the latter cases, the use of intravenous artemisinins has given better results than the administration of intravenous quinine. In pregnant women in highly endemic areas, a prophylactic dose of sulfadoxine-primetamine should be administered to eliminate possible parasites present in the placenta..
In the event of any suspicion of malaria, the patient should be taken to a medical center for parasitological confirmation. Treatments based exclusively on clinical pictures are only indicated in the absence of immediate tests and their results.
It is advisable to administer antimalarial drugs within the first 24 hours to prevent complications..
The World Health Organization establishes the following basic principles for the prevention of malaria:
Given the importance in public health worldwide, the WHO has proposed important strategies and programs. Among which stand out the Global Technical Strategy against Malaria 2016-2030, a technical framework for all countries where malaria is endemic, and the World Malaria Program, an instrument that seeks to coordinate global activities linked to the Organization to fight against malaria, among others.



Yet No Comments