The promonocyte it is an intermediate stage between the monoblast and the monocyte during the process of cell differentiation and maturation called monocytopoiesis. It is an immature cell that under normal conditions is scarcely found in bone marrow and absent in peripheral blood..
It is part of the mononuclear phagocytic system. It presents morphological characteristics that guide its recognition in bone marrow smears (under physiological conditions) or in peripheral blood of patients with certain types of leukemias.
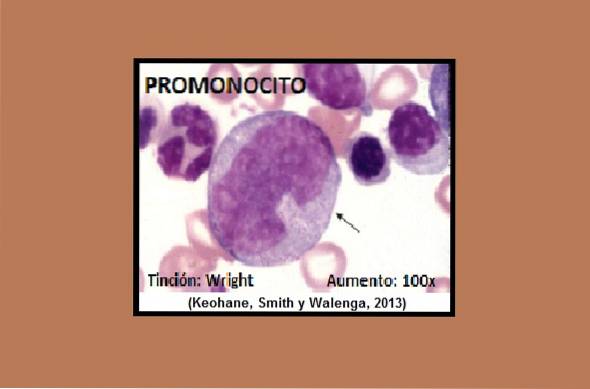
The promonocyte is basically a large cell with a high nucleus-cytoplasm ratio, measuring between 15 and 20 µm. Its nucleus presents a moderately lax chromatin, with 0 to 2 nucleoli. The cytoplasm is highly basophilic and sparse with a moderate presence of very fine azurophilic granulations.
However, it is difficult not to confuse it with the promyelocyte, an immature cell belonging to the granulocytic lineage, because they share many morphological characteristics..
That is why it is very common to use special cytochemical stains to detect the presence or absence of certain enzymes that help definitive identification..
Promyelocyte positive enzymes include peroxidase, acid phosphatase, and nonspecific esterases, such as α-naphthylbutyrate esterase and naphthol-As-D-acetate esterase..
As for the diseases that present with an increase in promonocytes in bone marrow and peripheral blood are acute myelomonocytic leukemia (M4), acute monoblastic leukemia (m5a, m5b) and chronic myelomonocytic leukemia.
These types of leukemias are usually very aggressive with a survival between 11 to 36 months.
Article index
The promonocyte is a cell that measures between 15-20 nm, with a spherical shape. The nucleus is prominent, eccentric and irregular, and may have a more or less pronounced notch. The nucleus is bounded by a thin film called the nuclear membrane..
In the interior of the nucleus a still lax chromatin is evident and sometimes it is possible to observe one or two nucleoli.
Its cytoplasm is scarce and rich in polyribosomes. With classic stains, the cytoplasm expresses its affinity for basic dyes, staining a grayish-blue color. In its interior, the scarce or moderate presence of azurophilic granules of violet color with an extremely fine appearance is notable..
It can often be confused with the promyelocyte with which it shares many morphological characteristics.
On the other hand, from the molecular point of view the promonocyte maintains some immunophenotypic membrane markers of the monoblast (previous stage), such as CD 33++ and the HLA-DR+, but it loses CD 34 and CD 38. And as new membrane antigenic markers it acquires CD 13+, CD 11b+ and the CD89.
The latter is also called the IgA Fc receptor; this receptor is important to stimulate the destruction of microorganisms through the induction of phagocytosis.
Promonocytes can sometimes be confused with promyelocytes. For this reason, for a more reliable identification, cytochemical stains can be used to help differentiate..
For example, promonocyte reacts positively with special stains to detect the following enzymes: peroxidase, acid phosphatase, arylsulfatase, α-naphthylbutyrate esterase, N-acetyl-ß-glucosaminidase, and fluorosensitive naphthol-As-D-acetate-esterase.
In this type of leukemia, more than 30% of the cells found in the bone marrow are blasts and more than 20% of the nucleated cells are of the monocytic series. A M: E ratio greater than 1 is observed; this means that the myeloid series is above the erythroid. It can occur with eosinophilia (M4-E).
In this leukemia there is a bone marrow with approximately 30% blasts and of these, 80% correspond to cells of the monocytic series. While the cells belonging to the granulocytic lineage are diminished (< del 20%).
This leukemia is divided into two, the m5a and the m5b. In m5a, the monocytic series is represented by the almost exclusive presence of monoblasts (> 80%), therefore it is called poorly differentiated. Monoblasts are abundant in peripheral blood and it has a very poor prognosis; usually present in young patients.
While the m5b < del 80% de la serie monocítica está presente en médula ósea corresponde a monoblastos y en cambio hay mayor cantidad de promonocitos y monocitos; por esta razón es llamada leucemia diferenciada. En sangre periférica hay un aumento significativo de monocitos circulantes.
As part of the diagnosis, it must be taken into account that in this pathology the lysozyme enzyme is found at quite high levels.
This disease is diagnosed when a constant high number of mature monocytes is observed in the peripheral blood for more than 3 months; as well as eosinophils.
Chronic myelomonocytic leukemia can be classified into 1 and 2, depending on the percentage of immature cells present in the peripheral blood and in the bone marrow..
Type 1 is characterized by presenting a percentage of immature cells less than 5% in peripheral blood and less than 10% in bone marrow.
While in type 2 there is presence of more than 5%, but less than 20% of immature cells in peripheral blood, and between 10-20% in bone marrow.
Among the immature cells present in peripheral blood is the promonocyte, together with monoblasts and myeloblasts.
In addition, there is an absence of the Philadelphia chromosome, which rules out chronic myeloid leukemia. Dysplasia may be present in other cell lines, that is, abnormal growth may be seen in red blood cell and platelet precursors.
It especially attacks adults or the elderly.
This rare pathology is caused by a mutation in the GATA2 gene. It is characterized by the partial or total absence of the monocytic cell series in peripheral blood, as well as other cells such as NK lymphocytes, B lymphocytes and dendritic cells..
These patients are at high risk for opportunistic infections and malignancies. It is considered an immunodeficiency disorder, and treatment focuses on bone marrow transplantation.



Yet No Comments