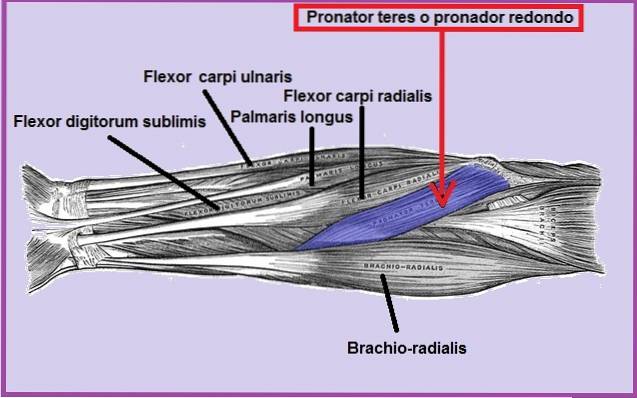
The round pronator is a muscle of the forearm, also known by the name of musculus pronator teres or radii teres. It is a flattened muscle, positioned obliquely and superficially on the anterior and proximal part of the forearm..
This muscle is innervated by the median nerve and supplied by the ulnar artery and the radial artery. Knowing the path, not only of the muscle but also of the median nerve, is essential to be able to offer adequate treatment, especially when there is compression of the nerve and the pain radiates from the forearm to the hand..
This muscle is very useful, since it allows the forearm to rotate, called pronation. Therefore, those activities or sports that have as their main movement the rotation of the wrist and forearm repeatedly, can affect the pronator teres muscle..
For example, the movement that golfers, baseball players and javelin throwers must make in their respective sports.
Article index
Muscle comprises two bundles of muscle fibers, also called fascicles. The thickest comes out of the bony bump. The latter is located on the inside of the elbow, just above the trochlea, that is, the medial epicondyle of the humerus or epitrochlea..
Whereas, the thinnest fascicle originates from the protrusion of the ulna, called the coronoid process of the ulna..
The pronator teres muscle is implanted towards the distal and lateral area of the radius, specifically in the middle third.
The pronator name comes from the word pronation, from the Latin pronatio. The term pronation means rotation, in this case of the forearm. Therefore, the name of the pronator muscle refers to its function.
The pronator teres accompanies the pronator square in the rotary movement. Both muscles manage to position the forearm with the back of the hand up. This movement is called pronation. It also allows the forearm to flex upward..
The opposite movement, where the back of the hand is down is called supination and is carried out by other muscles.
It should be noted that the pronator teres is a helper or secondary muscle, since the pronator quadratus is the main muscle in pronation. The pronator teres muscle reaches its greatest power when the arm is stretched.
The musculus pronator teres or pronator teres is innervated by the median nerve. This is located between the two muscle fibers of the pronator muscle.
The muscles must be irrigated with blood in order for them to function properly. In this sense, the pronator muscle is supplied by the ulnar or ulnar artery and by the radial artery.
It was first described by Seyffarth. It occurs when the median nerve is compressed for some reason.
The nerve can be compressed by various causes, including congenital anomalies, trauma, muscle hypertrophy, tumors, among others. These causes can produce anatomical displacement of its path and cause compression of the same..
Normally, the nerve leaves the ulnar fossa and continues its journey passing between the two heads of the pronator teres muscle (ulnar and humoral)..
However, Rivero et al. Found that sometimes the median nerve can have other routes and pass behind the heads of the muscle fibers of the pronator teres or behind one of the heads (ulnar or humoral) of the same muscle..
Other times the median nerve can be found piercing the ulnar head of the pronator teres..
The nerve can also be compressed when it passes through the fibrous arches. These are formed by the superficial flexor muscle of the fingers and the pronator teres muscle, or even both..
On the other hand, it is possible that the median nerve is compressed at the elbow (supracondylar area), due to the presence of the Struthers ligament. This ligament is only present in 2% of the population. The affectation is called Struthers syndrome..
All these changes can cause pain in the forearm and hand. Sometimes there may be weakness in the movements of the thumb (thumb opposition), loss of strength and paresthesia (impaired sensation).
When pronator syndrome is accompanied by carpal tunnel syndrome, the clinical picture is called double compression syndrome..
Treatment of pronator syndrome will depend on the cause. Most of the time it resolves with rest, but in other cases surgical decompression is necessary.
It is produced by compression of the branch of the median nerve that supplies the wrist, called the cutaneous palmar branch. Thickening, trauma, and inflammation of the wrist tendons can narrow the carpal tunnel and compress the nerve.
This can be caused by other conditions, such as rheumatoid arthritis or by the excessive use of flexion and movement of the wrist. For example, people who work for hours typing on a computer and use the mouse excessively.
Women are more likely to suffer from carpal tunnel syndrome than men. Symptoms are numbness, tingling, and pain in the hand and fingers. Pain can sometimes radiate to the forearm.
Treatment may involve rest, splinting, ice, oral anti-inflammatories, and ultimately surgical treatment..
Epicondylitis is a very painful condition at the elbow. It is produced by excessive rotational movements of the forearm. There are two types, lateral and medial epicondylitis..
The first is very common in tennis players, which is why it is popularly known as "tennis elbow", while the second is very common in those who practice golf or baseball, therefore, the affectation is often called " golfer's or baseball's elbow ”.
Medial epicondylitis occurs due to involvement of the pronator teres muscle, although the flexor carpi radialis and palmaris longus may also be involved..
For this, several maneuvers can be performed. Among them is the pronator teres compression test. This test shows if there is an involvement of the median nerve.
The test consists of sitting the patient and facing him. The patient's elbow is slightly flexed (20 ° - 45 °) approximately. The doctor holds the patient's elbow with one hand and takes his hand with the other. The patient is asked to try to extend and rotate the forearm, while the physician resists the movement.
The patient may also be asked to permanently rotate the forearm with force, without the forearm being blocked by the examiner..
Another maneuver that can be performed is to resist the rotation and flexion of the wrist. Finally, the index, ring, and little fingers are extended while the patient tries to bend the middle finger toward himself. This last test is usually painful and annoying on its own.
All the mentioned tests are interpreted in the same way. A test is positive when the patient during the test experiences a paraesthetic sensation along the entire path of the nerve.
Electromyography is not helpful in diagnosing pronator syndrome. Whereas, radiography is only useful in the presence of the Struthers ligament.
For its part, ultrasound is of little use unless there is a tumor, hypertrophy or hematoma that may be causing compression of the median nerve.
Lastly, MRI gives very good results, but it has the disadvantage of being very expensive.


Yet No Comments