
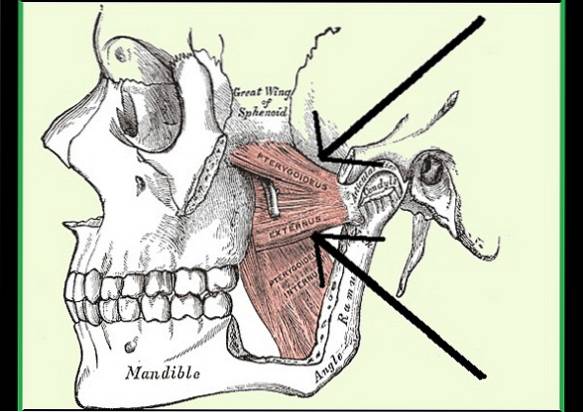
The external pterygoid or lateral pterygoid is an important chewing muscle. The term comes from the Latin Pterygoideus lateralis or externus. It is composed of two fascicles or muscle bundles, one upper and one lower. Each muscle bundle fulfills a specific function contrary to that of the other, but they work in a coordinated way..
The lower fascicle is responsible, along with other muscles, for opening the mouth and making movements of the jaw forward and to the sides. While the superior fascicle does the opposite, it acts to close the mouth and return the jaw to its original or resting place.
This muscle begins to form in humans around the 10th week of embryonic development and culminates in its formation around the 20th week of gestation..
The external pterygoid can suffer from tension spasms of various causes and cause pain. It is also believed that the spasm of this muscle is the cause of other pathologies such as pain syndrome and temporomandibular joint dysfunction..
Article index
It is a small, triangular-shaped muscle whose anterior insertion is located under the skull and its posterior insertion is positioned in the temporomandibular joint. The muscle encompasses the roof of the pterygomaxillary fossa.
It is a paired muscle, as there is one on each side of the face symmetrically. The lateral pterygoid muscle is covered by a thin aponeurosis called interpterigoid (Fasciae inter pterygoideus) and for the pterygoid aponeurosis.
The external pterygoid muscle has three faces: a superior face, an anteroexternal and a postero-internal.
It delimits with the greater wing of the sphenoid (vault of the zygomatic fossa). It should be noted that there are several nerves between the muscle and the aforementioned structure, including the masseteric nerve, the medial deep temporal nerve, the buccal nerve and the branches of the lower jaw.
It delimits with the masseter muscle (sigmoid notch), with the coronoid process, the temporalis tendon and with the bags of Bichat.
On this side it delimits with the internal pterygoid muscle, the lingual nerve, the inferior dental nerve and the auriculotemporal nerve..
This muscle has two fascicles, called the sphenoid or superior bundle and the pterygoid or inferior bundle. However, there are authors who describe a third part located in the lower part of the pterygoid bundle. Each one originates from a different site.
The sphenoid or superior bundle (smallest fascicle) arises from the greater wing of the sphenoid bone through its horizontal infralateral portion, and medial to the sphenoid or temporal crest of the sphenoid. Its fibers are arranged outwards and backwards horizontally until they reach the insertion site.
For its part, the pterygoid or inferior bundle (larger fascicle) originates in the pterygoid process (wing and external face), in the palatine bone (external part of the pyramidal process) and in the tuberosity of the maxillary bone.
A part of its fibers (the lower ones) are arranged outwards, up and back and the other part of its fibers (the upper ones) are directed outwards and up until they reach the insertion site..
Both fascicles are directed towards the temporomandibular joint (TMJ) or craniomandibular joint complex. The inferior fascicle attaches to the inner part of the condyle of the mandible, specifically in the pterygoid fossa.
Whereas, the superior fascicle inserts into the interarticular disc of the TMJ and for this it penetrates the joint capsule. Also a part is inserted into the deep fibers of the pterygoid or inferior bundle.
The external or lateral pterygoid muscle is irrigated by the internal maxillary artery or also known as the internal mandibular artery, this will emit ascending as well as descending branches.
Some authors mention another artery called interpterigoid artery that may come from the same internal maxillary or middle meningeal branch..
The external pterygoid muscle receives innervation from an external branch belonging to the mandibular nerve, called the temporobucal nerve.
It is a muscle that acts in the chewing process. The lower and upper portions work separately but coordinated, in such a way that each one has a function and when one is active the other is inactive and vice versa..
The inferior fascicle contracts together with other muscles when we open our mouth and also when we move the jaw laterally (ipsilateral mandibular movements) or forward (protrusion movement), outside its normal limits voluntarily. During these movements the upper part is inactive.
The superior fascicle is activated when we close the mouth and when we return the mandible to the original position, that is, during the retrusion movement (backwards) and in the stabilization of the TMJ joint to the medial position. In this case, the inferior fascicle becomes inactive.
That is why, it is said that this muscle performs a stabilizing function of the temporomandibular joint, specifically of the head and condylar disc..
The causes that can cause this muscle to tense are abnormal occlusion, stress, anxiety or rage attacks and trauma.
When there is pain in the jaw area, it is difficult to determine which muscle is affected. One way to find out is to ask the patient to try to clench the teeth, if this increases the pain, it means that the muscle involved is the superior pterygoid..
However, intracapsular pain causes the same discomfort when performing this exercise, therefore, to differentiate both pains, the patient is now asked to clench the teeth but placing a spacer between them, if the pain persists it comes from the muscle, but if the pain decreases, then it is intracapsular pain.
On the other hand, if we ask the patient to open his mouth as wide as possible and that does not cause discomfort, it means that the lower fascicle is not affected, but if it hurts, then it is involved..
This condition is also called temporomandibular joint pain and dysfunction syndrome (TMDJS). When there are problems with the temporomandibular joint, consider checking the external pterygoid muscle..
Anterodiscal displacement of the joint could be associated with a spasm of this muscle.
Myofascial pain that occurs in this muscle usually radiates to the jaw and ear.
This muscle is very difficult to palpate and even more so if the patient feels pain. One possible treatment is dry needling of the external pterygoid. There are also exercises that help stabilize the jaw, but they must be guided by specialists.
If there is anterior dislocation in the disc with reduction, therapies can be performed to regain the position of the disc, but this is only possible after having worked with stretching exercises to the external pterygoid muscle..



Yet No Comments