Bengal rose It is a laboratory test based on an antigen-antibody reaction for the diagnosis of brucellosis. The technique allows detecting specific antibodies against the bacteria Brucella abortus in human serum samples. The result can be reported qualitatively or semi-quantitatively.
The qualitative form expresses whether the patient is positive or negative for the test, that is, whether or not there are antibodies. Meanwhile, the semi-quantitative report is reported in IU / ml and indicates the approximate amount of antibodies present. It should be noted that antibodies will only be produced if the patient has been in contact with the microorganism.
Due to its great simplicity, high sensitivity and specificity, it is one of the seroagglutination techniques most used in medicine as an initial test for the diagnosis of this disease..
Some researchers have compared the efficacy of the Rose Bengal test with other techniques, such as seroagglutination (febrile antigens) and have observed that although there is good correlation, they saw isolated cases in which the febrile antigen test was negative and Rose de Positive flare.
The difference obtained was due to the fact that these patients had a subclass of IgG antibodies against Brucella abortus with better binding capacity at acidic pH, therefore they could react with the Rose Bengal reagent but not with that of febrile antigens.
In this sense, they have suggested that the reagents of the febrile antigen technique be modified to an acidic pH so that they can detect this type of cases..
Article index
The Rose Bengal Reagent consists of an antigenic suspension. It is made up of the S99 strain of Brucella abortus, diluted in an acidic lactate buffer (pH 3.6), plus phenol and the Rose Bengal dye.
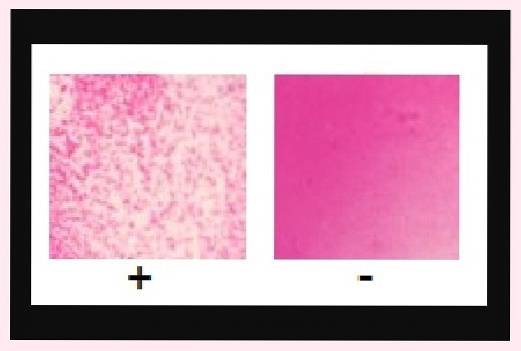
Therefore, in the sample what is sought are anti-Brucella antibodies, if these are present they will react with the reagent antigen and a macroscopically visible agglutination reaction will be observed. The test detects either IgM antibodies or IgG antibodies.
This means that it can detect the disease both in its acute stage where IgM antibodies prevail or in its chronic stage where IgG antibodies predominate..
This represents an advantage since it increases the sensitivity of the test but at the same time it is a disadvantage since it does not discriminate between one stage and another, because the reaction with IgM and IgG antibodies are identical.
The test must always be performed together with a negative control and a positive control. The negative control contains animal serum without antibodies and the positive control contains serum of animal origin with 50 IU / ml of anti-Brucella antibodies..
Brucellosis is a serious disease that tends to be chronic and dangerous, so it is very important that it be diagnosed early. It is a zoonosis and humans can be infected by direct contact with contaminated material, the most vulnerable people being veterinarians and animal caretakers..
Infection can also occur by consuming infected raw meats, among other forms of contagion.
This disease attacks locally or systemically. The systemic form is the most serious, since various organs can be affected, including the reticulum endothelial system (liver, spleen, bone marrow), skin (cellulitis and lymphadenopathy), respiratory system (pneumonia), musculoskeletal system (arthritis, sacroiliitis and spondylitis), among others.
The Rose Bengal test is a very useful technique to carry out an initial screening, because it is very inexpensive, easy to use and with great specificity and sensitivity..
Cases of false negatives and false positives are very rare, and can occur in people with very low antibody titers (< 25 UI/ml) o extremadamente altos (>1000 IU / ml) respectively.
-Rose Bengal Kit
-Agglutination plate white background
-50 µl pipette
-Rotator (optional)
-Vortex
Rose Bengal commercial kits come with ready-to-use reagents.
-Temper reagents before starting work.
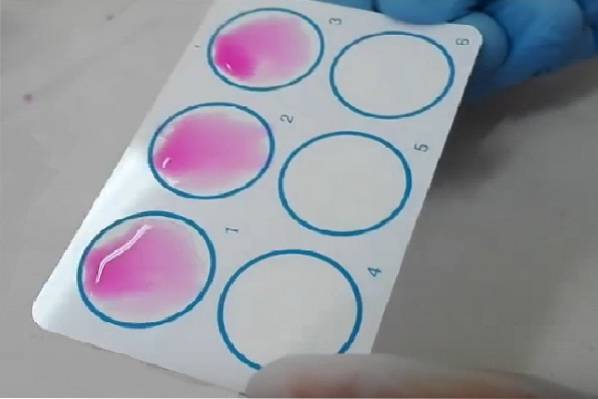
-The agglutination plates have circles drawn, each one for a different sample. Use 3 circles, the first for the negative control, the second for the sample and the third for the positive control.
-Place a drop or 50 µl of the controls and the sample in their corresponding circle.
-Mix the Rose Bengal Reagent using a vortex. Place a drop next to the previously placed ones.
-Mix with wooden toothpicks (use one for each specimen or control). Make circular movements and spread in such a way that it covers the entire circle.
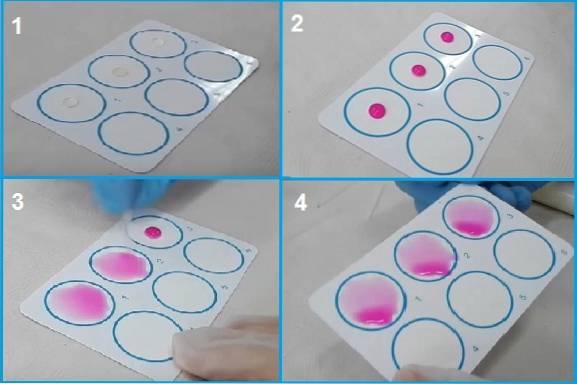
-Place the plate on an automatic rotator at 80 to 100 RPM or rotate manually for 4 minutes. Read the proof at the end of this time.
-Verify that the controls gave as expected. Compare the reaction of the test sample with the controls. Report as positive if agglutination is observed and as negative if there is no agglutination.
A positive test indicates that the patient has an amount equal to or greater than 25 IU / ml of anti-Brucella antibodies.
If in the qualitative reaction the sample is strongly positive, it can be semi-quantified. For this, serial double dilutions of the sample are made with physiological saline solution. The procedure described above is carried out with each dilution..
It is also interpreted by observing the agglutination macroscopically. The result will be the titer of the highest dilution in which a positive result was observed.
To calculate the approximate value of anti-Brucella antibodies, the following formula is used:
25 IU / ml x reaction titer = IU / ml
Example, if a patient in the semi-quantitative test tests positive at the ½, ¼ and 1/8 dilution and begins to be negative from the 1/16 dilution onwards, this means that the patient has a titer of 8.
Applying the formula:
25 IU / ml x 8 = 200 IU / ml
-The kits have an expiration date and it must be respected. Should not be used if the reagent is expired.
-During use, make sure that the reagent does not contain solid particles, as this is a sign of deterioration..
-Store between 2 and 8 ° C.
-Do not freeze, this act irreparably damages the reagent.
-Always run the test together with the negative and positive controls.
-The technique tolerates serum samples with a certain degree of lipemia and hemolysis, however it is not advisable to use exaggeratedly lipemic and hemolyzed sera, both conditions alter the results of the test..
-Always warm the reagents to room temperature before starting the analysis..
-Do not interpret reactions that take more than the recommended time, as this generates the report of false positives, since after a certain time the reagent precipitates, simulating a positive reaction.
-The technique is 100% sensitive and has a specificity of 98%.
-After a semi-quantification of 1000 IU / ml there is the possibility of observing a prozone effect (false negative due to excess antibody compared to the amount of antigens).



Yet No Comments