
The salpingoclasia it is a sterilization method for women. It is generally permanent, depending on the technique used. Classically it involves an operation of the fallopian tubes that must be performed with a wedge incision at the level of the horn of the uterus and the closure of the wounds with sutures.
"Salpingo"Means horn and"classia”Is a suffix that means crushing or breaking. Literally, salpingoclasia means the crushing or breaking of the tubes, in this case, the fallopian tubes..
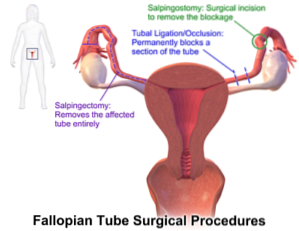
There are several synonyms for this procedure such as tubal ligation, bilateral tubal occlusion (OTB), tubal sterilization, and tubectomy. The ultimate goal of this procedure is to interrupt tubal patency (of the fallopian tubes) and thus prevent fertilization of the ovum and implantation of the egg..
Sterilization as a contraceptive method is a choice for millions of men and women of reproductive age. Among women who use any contraceptive method, a third of them rely on male or female sterilization.
The procedure is indicated for those who request it and who really understand that it is generally an irreversible process. Reversing this sterilization procedure is difficult and very unsuccessful. It is generally used in people who have already procreated and do not want to have more children.
Before undergoing sterilization, people should receive advice to study other alternatives and learn about the pros and cons of this procedure. Not recommended for very young women.
The sterilization process in women usually consists of the occlusion, excision or division of the fallopian tubes. The procedure can be performed after a vaginal delivery or cesarean section, or by an elective intervention unrelated to the puerperal period (postpartum period)..
There are some medical conditions in which a pregnancy can put a patient's life at risk. For example, in patients with severe congenital cardiovascular disease, these simple, low-complication methods may be a good choice..
Article index
There are several techniques to interrupt tubal patency. Generally a segment of the middle portion of each tube is excised (cut).
Each end is cauterized with an electrosurgical knife or sutured, and is completely sealed by fibrosis and peritoneal regrowth. Other methods use the implantation of rings that seal the tubes.
In the case of puerperal salpingoclasia, it can be done directly in the course of a cesarean section. If it is done after vaginal delivery, it can be done immediately after delivery or in the puerperium, 1 to 3 days after delivery..
The advantage of performing the intervention in the puerperal period is that for several days after delivery, in the mediate puerperal period, the fundus of the uterus (upper part of the body of the uterus) is at the level of the navel and the tubes are directly accessible below of the abdominal wall, which facilitates access to the tubes.
If an epidural catheter was used for analgesia during labor, it can be used for sterilization analgesia. Good bladder emptying must be ensured, usually with a urethral catheter. This prevents bladder injuries during the intervention and the removal of the uterine fundus above the navel.
A small infraumbilical incision is made that follows the curve of the belly button so as not to leave visible unsightly scars. One of the reasons why these interventions can generate failures is due to the wrong ligation of the round ligament instead of the sectioned tube.
If the intervention is not related to the puerperium, several techniques and several access routes can be used.
Some routes are laparoscopic and consist of two small incisions of 1 cm each, made at the edge or upper limit of the pubic hair. To do this, and in order to expand the space and avoid injuries, a gas is first injected into the cavity.
Then a laparoscope is inserted, which is a thin tube with an optical fiber that allows you to visualize the procedure. Through the other incision, a trocar (a kind of awl covered with a cannula) is introduced through which the instruments are introduced..
This procedure can be performed under general anesthesia or with local anesthesia and sedation..
Another route is a surgical intervention under general anesthesia and an incision of about 5 cm in the pubic area. This is done taking advantage of some other surgical procedure that must be performed on the patient.
The tube can also be accessed through the cervix and a kind of spring is placed inside the tube. The method is called “esurre " and it is a permanent and irreversible method. Before performing any of these procedures, the absence of pregnancy must be verified.
Many techniques have been developed for these types of procedures that can be grouped by the type of occlusion media used. There are methods with surgical resection and ligation, occlusion with staples, clips or rings, electrocoagulation methods and excretion..
The means of occlusion of the patency of the tubes can be by surgical resection and ligation, among which the Parkland, Pomeroy and modified Pomeroy techniques can be mentioned. They are the most widely used because they have few failures and very few complications.
Other methods of tubal occlusion use staples or clips with different shapes and materials. Silicone rings are also used. These procedures can cause compression necrosis of the local tube circulation..
There are also methods that use electrocoagulation, that is, those that let a small electrical current pass in order to burn a small portion of the tube..
Finally, a method that is very popular due to the ease with which it can be performed, since it does not need anesthesia, or incisions, or ligatures, and because of its high effectiveness, consists of placing a micro-insert in the tubes vaginally through the cervix. to the tubes and the implantation is done.
The body generates an inflammatory process around the implant that closes the tubes and after three months a fibrotic tissue develops that permanently closes the tubal duct.
In underdeveloped countries that have high birth rates and where economic problems prevent women from accessing other contraceptive methods, outpatient sterilization campaigns for multiparous women have been effective in reducing birth rates in very low-income families and with important family responsibilities.
- Its contraceptive effectiveness is immediate, with the exception of esurre, which takes three months to guarantee contraception.
- You can have an active sex life without danger of pregnancy.
- His recovery is very fast, seven days at the most.
- Does not alter hormonal secretions.
- Does not alter menstrual cycles.
- Some techniques do not require incisions or anesthesia.
- Lowers the risk of ovarian cancer.
- As the procedure is practically irreversible, aspects related to the couple must be considered, the future possibility of a divorce and of having another partner and wanting to procreate, the loss of a child, etc. Psychological support is very important for such a momentous decision.
- Some women express remorse or regret for being sterilized, especially when the procedure was performed at a very young age. For this reason, some gynecological schools do not recommend this procedure before the age of 30 unless there are medical causes that indicate it..
- As the reversal process is very complicated and ineffective, if you want to have another child, you will probably have to resort to in vitro fertilization.
These procedures have few side effects, however, pain and discomfort may occur during the procedure and in the first few days after..
Like any surgical procedure, salpingoclasia can have some risks such as vascular or urinary bladder damage during the intervention, serious infections due to perforation of the intestinal viscera during the surgical procedure, etc..
Due to some defects of the surgery or due to the formation of a fistulous tract or a spontaneous reanastomosis of the sectioned tube, pregnancy can occur. Generally and depending on the method used, this possibility affects between 4 and 7 of every 1000 women subjected to sterilization..

One of the most important and common side effects after tubal reanastomosis are ectopic pregnancies, that is, the implantation of a fertilized egg outside the uterus. This situation is a surgical emergency that puts the mother's life at serious risk..
The use of the different intratubal implants vaginally through the cervix has been associated with some complications such as abnormal bleeding, uterine or fallopian tube perforation due to implant migration, allergies or hypersensitivity reactions, especially to the components nickel.
Some events of this nature have required abdominal surgery to remove the device. As initially the blockage of tubal patency with implant methods is not 100%, it is necessary to confirm it three months after the procedure with an examination called hysterosalpingography..
Hysterosalpingography is a radiological test used to examine the uterus and tubes, using fluoroscopy and contrast. With the confirmation of the closure of the tubes, the effectiveness of this method amounts to 99%.


Yet No Comments