Staphylococcus haemolyticus it is a Gram positive coconut-shaped bacterium. It is an integral part of the normal microbiota of the skin in humans, primates and domestic animals. It falls under the classification of coagulase negative Staphylococcus and until recently it was not mentioned much.
However, this species has become important, because it has been isolated from a wide variety of clinical samples. In recent times, its great capacity to acquire resistance to antibiotics commonly used in hospitals has been studied.
This has increased the numbers of nosocomial infections and with it the morbidity and mortality rate caused by coagulase-negative Staphylococcus. In some health centers, endemic strains causing bacteremia have been isolated in intensive care units.
These infections are probably due to the contamination of prosthetic materials such as heart valves, vascular grafts, pacemakers, intracranial pump implants, mesh, breast, joint or penile prostheses..
Also due to contamination of medical devices such as venous catheters, CSF shunt, peritoneal dialysis catheters, urinary catheters, suture material, among others..
It affects immunosuppressed patients, especially neutropenic patients and newborns. However, infections by Staphylococcus haemolyticus They can be of nosocomial origin or of community origin. That is, it is viable in both environments..
Article index
-Staphylococcus haemolyticus it is a facultative anaerobic microorganism, it is not mobile and does not form spores.
-It grows well in blood-enriched culture media from 18 ° C - 45 ° C. With an optimum temperature of 37 ° C.
-It is characterized by giving a negative reaction to the coagulase, urea, ornithine decarboxylation and phosphatase test.
-Reacts positively to: test for catalase, nitrites, arginine, pyrrolidoni-larylamidase (PYR).
-In relation to the formation of acids from carbohydrates, it is distinguished by being an acidifier of glucose, maltose, trehalose and sucrose..
-It can give variable results against lactose, fructose, ribose and mannitol, and does not ferment mannose, raffinose, cellobiose, arabinose and xylose.
-Against the antimicrobials used for diagnostic purposes polymyxin B and novobiocin, it behaves as sensitive, and against bacitracin as resistant.
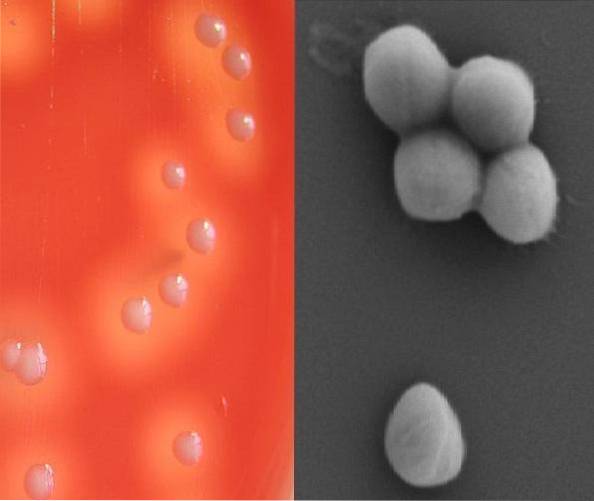
They are cocci that under Gram stain stain purple, that is, they are Gram positive.
Its distribution in space is like that of any staphylococcus, that is, in clumps simulating bunches of grapes. They have a size between 0.8 to 1.3 µm in diameter.
Macroscopically, the colonies on blood agar are creamy white and produce ß-hemolysis around the colony. See left side image in article introduction.
Staphylococcus haemolyticus has teichoic acid in its cell wall and can produce a polysaccharide capsule.
Domain: Bacteria.
Phylum: Firmicutes.
Class: Bacilli.
Order: Bacillales.
Family: Staphylococcaceae.
Genus Staphylococcus.
Species: haemolyticus.
One of the main problems it presents S. haemolyticus it is the ability to acquire antimicrobial resistance genes, which complicates the clinical pictures.
Likewise, this species plays an important role in the dissemination of resistance genes, contributing to the appearance of different, more virulent epidemic clones..
This microorganism has reported high resistance to methicillin.
It is known that the methicillin resistance mechanism in Staphylococcus determines resistance to all b-lactam antibiotics: penicillins, cephalosporins, carbapenems and monobactams.
This resistance is mediated by the overproduction of PBP-2a, an altered penicillin-binding protein with low affinity to ß-lactam antibiotics and which is encoded by the gene mecca.
Likewise, high resistance has been seen to other groups of antibiotics such as ciprofloxacin, erythromycin and gentamicin. Meanwhile, it responds very well to linezolid and rifampin, followed by trimethoprim - sulfamethoxazole and vancomycin..
For vancomycin, important cases of heterogeneous resistance have already been reported. This has hampered successful treatment in neonatal, neutropenic, and intensive care patients..
Resistance to glycopeptides results from the acquisition and expression of operons that substitute a terminal D-lactate or D-serine for D-alanine, which reduces the binding affinity to vancomycin.
Staphylococcus haemolyticus it is especially predisposed to resistance to glycopeptides, due to its extraordinary plasticity of the genome and tendency to frequent DNA rearrangements.
Confers resistance against phagocytosis.
It has been seen that S. haemolyticus it is capable of forming biofilm in venous catheters and prostheses. This property increases resistance to antibiotics by acting as an impermeable barrier, prolonging and complicating infectious processes..
This property is increased in capsulated strains and in the presence of glucose and NaCl in the medium..
100% of the strains produce hemolysins, which are evidenced by a clear halo around the colonies on lamb blood agar, while only some can produce enterotoxins.
Some strains are produced by others not.
Among the pathologies that Staphylococcus haemolitycus originates are: Bacteremia, wound infection, diabetic foot, osteomyelitis, post-surgical ophthalmic infection, endocarditis, meningitis.
In a study carried out at Hospital II of Chocope Peru, strains of Stpahylococcus haemolitycus from various sources obtaining a recovery percentage as follows:
Vaginal discharge 25%, sperm 25%, vertebral discharge 20.8%, pharyngeal discharge 16.7%, urine 8.3%, wound 4.2%.
Other researchers carried out a similar study in Paraguay and obtained: in urine 27.3%, purulent secretions (abscesses and wounds) 18.5%, blood cultures, catheter tip and bone 13.3%.
Likewise, another study revealed that 55.9% of babies within a hospital environment carried multi-resistant coagulase negative Staphylocococcus in their nasal cavity.
The most frequently isolated species were S. haemolyticus (38.3%) and S. epidermidis (38.0%).
On the other hand, multi-resistant strains of S. haemolyticus they also pose a serious problem in animal pathology, since they have been isolated from both ruminants and domestic animals.
Therefore, there is a great possibility of transmission between animals, their owners and veterinarians. Animals can act as reservoirs for strains of S. haemolyticus multi-resistant.
What's more S. haemolitycus could be the reservoir of resistance genes for other staphylococci, including S. aureus.
Coagulase negative Staphylococcus strains including Staphylococcus haemolyticus can be identified with the semi-automated MicroSscan® or ALPI-Staph (Biomerieux ©) system to name a few.
This system allows the identification of Staphylococcus species by means of:
All this after 16-48 hours of incubation at 37 ° C.
In venous catheter infections, the possibility of removing it should be considered, if this is not possible then it should be sealed.
Concomitant with this, antibiotic therapy with vacomycin, linezolid or daptomycin should be administered. The use of cloxacillin is restricted to strains that are sensitive to methicillin..
In the case of prosthetic infections, a prolonged treatment should be administered, combining rifampicin and a fluoroquinolone or linezolid..
This treatment almost always avoids the need to remove the prosthesis. However, if the infection does not subside, it should be removed..
In meningitis and postsurgical endophthalmitis, it can be treated with linezolid.



Yet No Comments