Staphylococcus saprophyticus It is a bacterium that is part of the group of Staphylococcus called coagulase negative. It is a microorganism of clinical importance, as it causes urinary infections mainly in young pregnant or sexually active women..
While other coagulase negative Staphylococcus can cause nosocomial infections in immunosuppressed hospitalized patients, Staphylococcus saprophyticus it mainly affects healthy women in the community. In addition, it is the second most common cause of cystitis after Escherichia coli.
Although it is generally present in less than 100,000 colony-forming units per milliliter of urine (CFU / mL), it is persistently detected in serial samples. That is why it is said that S. saprophyticus is a well documented pathogen.
The incidence of urinary tract infections S. saprophyticus it varies considerably between different patient populations and different geographic areas. It is usually related to recurrent infections and kidney stones.
Article index
Staphylococcus saprophyticus is a facultative anaerobic microorganism that inhabits the gastrointestinal tract of humans, with the rectum being the most frequent site of colonization, followed by the urethra, urine, and cervix.
It also inhabits the gastrointestinal tract of pigs and chickens. These can be transferred to humans through their consumption.
People colonized with this microorganism will not necessarily suffer from infections by this bacterium..
On the other hand, Staphylococcus saprophyticus differs from other coagulase negative Staphylococci in that it is almost always sensitive to most of the antibiotics used for urinary tract infections, with the exception of nalidixic acid and fosfomycin.
However, most strains are already resistant to penicillin and some to other beta-lactams. Strains with resistance to erythromycin, clindamycin, chloramphenicol and levofloxacin have been found.
Resistance to these antibiotics occurs mainly by two mechanisms: active expulsion pumps of the antibiotic and modification of the binding site of the antibiotic to the bacterial ribosome by methylation.
Among the biochemical characteristics that stand out in this microorganism are:
-It shows a negative reaction to the following tests: coagulase, decarboxylation of ornithine, reduction of nitraros to nitrites and xylose fermentation.
-While giving positive results in the following tests: Urea, Catalase, Maltose Fermentation and Sucrose.
-Some tests can give variable results such as lactose and mannitol fermentation and susceptibility to bacitracin, which can be sensitive or resistant.
-Likewise, it is sensitive to polymyxin B and resistant to novobiocin..
Coagulase negative Staphylococcus, including Staphylococcus saprophyticus, are morphologically similar to S. aureus and can share many of their virulence characteristics.
They are Gram positive cocci that are arranged in clusters. They are not motile, do not form spores and are not hemolytic.
Domain: Bacteria.
Phylum: Firmicutes.
Class: Cocci.
Order: Bacillales.
Family: Staphylococcaceae.
Genus Staphylococcus.
Species: saprophyticus.
The main virulence factor of this bacterium is its ability to specifically adhere to uroepithelial, urethral and periurethral cells in greater numbers than other Staphylocococcus..
So much is the tropism for the designated cells that they do not adhere to other cell types. This tropism for uroepithelial cells may partially explain the high frequency of urinary infections produced by this microorganism..
The enzyme urease, for its part, is an important virulence factor for other urogenital pathogens such as Proteus sp Y Corynebacterium urealyticum, where S. saprophyticus it is not far behind and is also capable of producing it.
Urease is a determining factor in the invasion of bladder tissue in animal models of urinary infection.
It has been shown that S. saprophyticus needs to be in the presence of urine and urease for a greater ability to produce extracellular matrix, that is, to form biofilm.
This explains recurrent urinary tract infections and, many times, therapeutic failure, since the bacterium, when it forms biofilms, is more resistant to the presence of the antibiotic..
This protein is associated with the surface of bacteria. It is called Ssp (for S. saprophyticus surface-associated protein). It is believed that this protein participates in the initial interactions with uroepithelial cells and, of course, in their adherence..
It is present on the surface of the bacteria but its role in the virulence of the microorganism is unknown..
Some strains show this characteristic and it seems to favor initial adherence to uroepithelial cells..
It is believed that the gateway to the urinary tract of young women is through intercourse, where bacteria can be carried from the vagina into the urinary tissue..
Other risk factors are: use of urinary catheters, pregnancy, benign prostatic hypertrophy, among others..
Patients with urinary tract infections usually present with dysuria, pyuria, and hematuria, with suprapubic pain. In patients with pyelonephritis, there may be fever, chills, tachycardia, and back pain..
Upper urinary tract infections (pyelonephritis) can occur in 41% to 86% of patients, and sometimes bacteremia can be seen from S. saprophyticus as a complication of an upper urinary tract infection.
On the other hand, this microorganism has been involved in urethritis in men and women (acute urethral syndrome), of urinary infections produced by catheters..
It has also been found in cases of prostatitis, epididymitis, bacteremia, sepsis, endocarditis and endophthalmitis
Likewise, it has been isolated from urinary tract infections in children and adolescents of both sexes in the absence of structural abnormalities of the urinary tract..
Cases of bacteremia and septicemia due to the administration of nutritional supplements by parenteral route contaminated with this microorganism have also been reported..
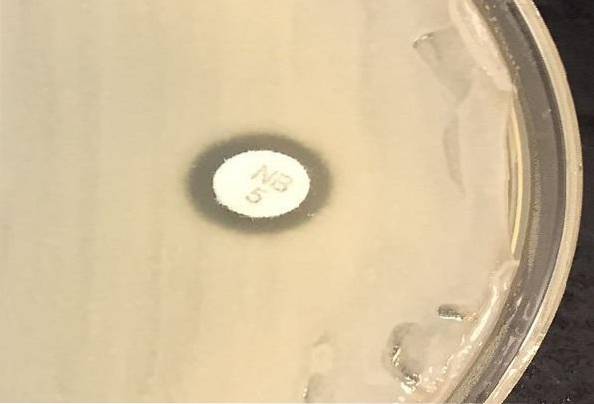
This species is resistant to novobiocin like S. cohnii, S. lentus, S. sciuri Y S. xylosus. But these last 4 species are rarely isolated from patients.
To find out if the strain is resistant or sensitive, the Kirby and Bauer technique is used. This consists of inoculating a Müeller Hinton agar plate evenly with a swab impregnated with the 0.5% McFarland bacterial suspension..
Subsequently, it is left to rest for a few minutes and a 5 µg novobiocin disk is placed. Incubate for 24 hours at 37 ° C. A zone of inhibition ≤16 mm indicates resistance. See image in introduction.
There are semi-automated methods that help to identify the microorganism, among them is the API STAPH-IDENT system. This system is quite good and has a lot of correlation with conventional identification.
Cotrimoxazole is an excellent option to treat cystitis caused by this microorganism, due to its pharmacokinetic and pharmacodynamic characteristics, as well as its tolerance and high urinary concentration..
Another option may be amoxicillin clavulanic acid, nitrofurantoin, and in complicated cases Trimethoprim-sulfamethoxazole..
In catheter infections, vancomycin or linezolid is useful..



Yet No Comments