The schizoaffective disorder is a mental disorder characterized by a mixture of symptoms of schizophrenia and mood disorders, either depression or bipolar disorder.
The appearance of symptoms usually occurs in early adulthood, occurring in less than 1% of the population. The causes appear to be genetic, neurobiological, and environmental, and may worsen with drug use.

The current main treatment is usually antipsychotics combined with antidepressants or mood stabilizers. To improve psychosocial functioning, psychotherapy and vocational rehabilitation are important.
The two types of schizoaffective disorder - both with some symptoms of schizophrenia - are:
In this article I will explain its symptoms, causes, treatment, consequences and more..
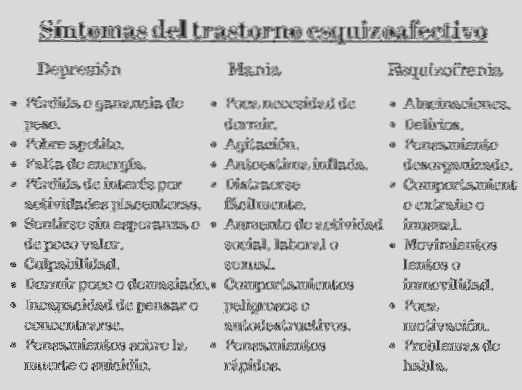
A person with schizoaffective disorder has serious mood swings and some psychotic symptoms of schizophrenia, such as delusions, disorganized thinking, or hallucinations.
Psychotic symptoms can occur when mood symptoms are not present.
The cause of schizoaffective disorder is thought to be a combination of environmental and genetic factors.
According to researcher Carpenter and colleagues, genetic studies do not support the view of schizophrenia, psychotic moods, and schizoaffective disorder as etiologically distinct entities.
According to these researchers, there is a common inherited vulnerability that increases the risk of these syndromes; some pathways may be specific for schizophrenia, some for bipolar disorder, and some for schizoaffective disorder.
Therefore, the genetic and environmental factors of a person interact in different ways to give rise to different disorders.
Specifically, schizoaffective disorder has been linked to advanced parental age, a known cause of genetic mutations..
It is difficult to prove a clear relationship between drug use and the development of psychotic disorders, however there is evidence of the specific use of marijuana.
The more cannabis is consumed, the more likely a person is to develop psychotic disorders, increasing the risk if used in adolescence.
A study of the Yale university (2009) found that cannabinoids increase symptoms of an established psychotic disorder and trigger relapses.
The two components of cannabis that cause effects are tetrahydrocannabinol (THC) and cannabidiol (CBD).
On the other hand, about half of people with schizoaffective disorder use drugs or alcohol excessively. There is evidence that alcohol abuse can lead to the development of a substance use-induced psychotic disorder.
Likewise, the use of amphetamines and cocaine can result in psychosis that can persist even in abstinent people.
Finally, although it is not considered a cause of the disorder, schizoaffective people consume more nicotine than the general population.
When a person is suspected of suffering from schizoaffective disorder, it is recommended to study the medical history, perform a physical examination and carry out a psychological evaluation.
The DSM-IV diagnostic criteria have caused problems by being inconsistent; when the diagnosis is made, it is not maintained in patients over time and has questionable diagnostic validity.
These problems have been reduced in the DSM-V. The following are the diagnostic criteria according to DSM-IV and DSM-V.
A) A continuous period of illness during which a major depressive, manic, or mixed episode occurs at some point, simultaneously with symptoms that meet Criterion A for schizophrenia.
B) During the same period of illness there have been delusions or hallucinations for at least 2 weeks in the absence of marked affective symptoms.
C) Symptoms that meet the criteria for an episode of mood disturbance are present for a substantial portion of the total duration of the active and residual phases of the disease.
D) The alteration is not due to the direct physiological effects of any substance or to a general medical condition..
Type-based encoding:
A. An uninterrupted period of illness in which there is a major mood episode (depressive or manic) concurrent with criterion A for schizophrenia. Note: the major depressive episode must include criterion A1.
B. Depressed mood. Delusions or hallucinations for more than two weeks in the absence of a major mood episode (depressive or manic) for the duration of the illness.
C. Symptoms that meet the criteria for a major mood episode are present for the majority of the duration of the illness.
D. The alteration is not attributable to the effects of one substance or another
medical condition.
Specify if:
The primary treatment for schizoaffective disorder is medication, which has better results combined with long-term social and psychological support..
Hospitalization can occur voluntarily or involuntarily, although it is currently rare.
Evidence suggests that exercise has positive effects on the physical and mental health of people with schizophrenia.
Medication is used to decrease symptoms of psychosis and mood. Antipsychotics are used for both long-term treatment and relapse prevention.
Atypical antipsychotics are advised because they have mood stabilizing activity and fewer side effects. Paliperidone is FDA-approved for the treatment of schizoaffective disorder.
Antipsychotics should be used in the minimum dose necessary to control symptoms as they can have side effects such as: extrapyramidal symptoms, risk of metabolic syndrome, weight gain, increased blood sugar, higher blood pressure. Some antipsychotics such as ziprasidone and aripiprazole are associated with less risk than others such as olanzapine.
Clozapine is an atypical antipsychotic that has been recognized as particularly effective when others have failed. It should also be considered in people with persistent suicidal thoughts and behaviors. Between 0.5 and 2% of people taking clozapine may develop a complication called agranulocytosis.
Control of the bipolar type is similar to that of bipolar disorder. Lithium or mood stabilizers such as valproic acid, carbamazapine, and lamotrigine are prescribed in combination with an antipsychotic..
For the depressive type, special attention should be paid if an antidepressant is prescribed, as it can increase the frequency of depressive episodes and mania..
For people who have anxiety, short-term anxiolytic drugs can be used. Some are lorazepam, clonazepam, and diazepam (benzodiazepines).
Psychotherapy can help - in combination with medication - to normalize the pattern of thoughts, improve social skills and reduce social isolation.
Building a trusting relationship can help the person better understand their condition and feel more hopeful. Life plans, personal relationships and other problems are also worked on.
Cognitive behavioral therapy (CBT) helps change negative thinking and behavior associated with symptoms of depression. The goal of this therapy is to recognize negative thoughts and teach coping strategies.
On the other hand, family or group therapy can be effective if the person can discuss their real problems with other people. Support groups can help reduce social isolation.
Electroconvulsive therapy may be considered for people experiencing severe depression or severe psychotic symptoms that have not responded to antipsychotic treatment..
People with schizoaffective disorder can have several complications:
It is estimated that schizoaffective disorder occurs in 0.5 to 0.8% of people at some point in their life, being more common in women than in men. This is due to the high concentration of women in the depressive subcategory, while the bipolar subtype has a more or less uniform gender distribution.
Some studies indicate that approximately 47% of people with this disease may be in remission after 5 years..
The prognosis depends on the functioning of the person before the onset of the disease, the number of episodes suffered, the persistence of psychotic symptoms and the level of cognitive impairment.
No, but if someone is diagnosed and begins treatment as soon as possible, it can reduce frequent relapses and hospitalizations, and decrease the interruption of personal life.
It is necessary to contact a professional if you, a family member or a friend experience:
And what experiences do you have with schizoaffective disorder?



Yet No Comments