The acromion It is a bone structure belonging to the shoulder blade, located in the lateral external extremity of this. It is a wide protrusion that sticks out in the shape of a paddle. It arises from the spine of the scapula, specifically from its outer posterior border.
It is said to be the outer part of the neck of the shoulder blade, while the inner part corresponds to the coracoid process. This bone piece has two faces (one upper and one lower), two edges (one medial internal and one lateral external), as well as a vertex.

The acromion together with the coracoid process and the coracoacromial ligament form the coracoacromial arch, graphically forming the roof of the subacromial space. The tendons that are part of the rotator cuff pass through there.
When the shoulder is in motion, the acromion should not rub against the muscles that line the glenohumeral joint, as doing so is the reason for the bursa and rotator cuff tendons to swell, weaken and tear, causing pain and limitation of movement.
The friction of the acromion with the tendons can occur due to trauma or degenerative diseases, both can cause the joint to start working incorrectly.
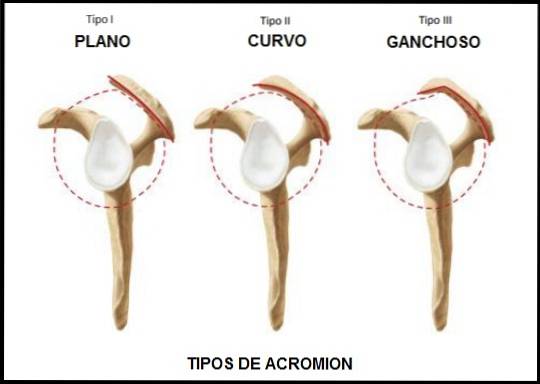
The shape of the acromion also has an influence, since they are flat, curved and hooked. On the other hand, it can present an abnormal ossification forming a spur. The latter is like a bone tumor that makes it difficult for the joint to move..
The term acromion comes from the Greek: akros, which means “taller” and ōmos “shoulder”. Sometimes it is also known as the acromion process.
Article index
The scapula, or shoulder blade, by its lateral external extremity has a protrusion that develops and thickens until it separates from the bone, called the spine of the scapula. Then that projection forms a kind of broad edge similar to a paddle and is called an acromion..
The acromion has several faces and edges: a superior face, a inferior face, an external or lateral border, a medial internal border and a lateral external extremity..
It has a rough surface full of holes or nutritional foramina through which blood vessels pass. It is convex in shape and lies just under the skin.
This face is concave in shape and smooth in appearance. It is just above the glenohumeral or scapulohumeral joint, separated by the subacromial space. When the distance of the subacromial space from the acromion is shortened, this face collides or rubs against the muscles above the joint (rotator cuff).
It is used for the insertion of some muscle fascicles of the deltoid (middle fascicles), therefore its surface is rough and thick, as it has 3 to 4 tubercles that allow a better grip for the muscle fibers.
It corresponds to the structure that articulates with the clavicle (external or acromial extremity of the clavicle) to form the acromioclavicular joint. For this reason, it has an elliptical center that fits perfectly with the clavicle. Both articular surfaces are covered by fibrocartilaginous tissue.
In this area there are ligaments that help their union, called acromio-clavicular ligaments (superior and inferior), although the union of these two structures is also strengthened by the coracoclavicular ligaments. This edge is shorter than the side edge.
It is the site of insertion of the acromiocoracoid ligament. This site is known as the vertex of the acromion..
They differ basically by the angle of the previous slope, which makes it change its shape.
It has an anterior slope angle of 13.18. It is the least frequent form found in the population (17.1%) and also the least involved in cases of patients with rotator cuff tear (3%).
In this case, the angle of the slope above is 29.98. It is the most commonly found in the population, with a frequency of 42.9%. This form of acromion is the second most related to rotator cuff tear (24.2%).
The angle of the slope above is 26.98. It is the second in frequency, found in 39.3% of cases, but it is the one with the highest percentage of association with cases of rotator cuff tear (69.8%). The hook shape increases the risk of rubbing against the muscles.
The acromion, together with the coracoid process, the coracoacromial ligament and fibers of the deltoid muscle, form a very important functional structure called the coracoacromial arch or acromiocoracoid vault..
If, in addition, two more structures are added, such as the scapular spine and the acromioclavicular joint, one is in the presence of the supraspinatus gorge.
The muscles and tendons of the rotator cuff slide through this area, which are closely related to the subacromial and subdeltoid bursae, also known collectively as the subacromyodeltoid bursa..
The acromion also serves as an attachment site for the deltoid muscle. It is also part of an important joint called the acromioclavicular (the junction between the clavicle and the acromion of the shoulder blade).
Finally shapes the shoulder.
When we are born, the acromion has 4 ossification centers called pre-acromion, meso-acromion, meta-acromion and basi-acromion, but at approximately 12 years the center called basi-acromion joins the scapular spine, while the rest of the ossification centers congregate among themselves, between the ages of 15 and 18.
However, in a small percentage of individuals (2%) there are abnormalities in which some of the ossification centers or several of them do not fuse..
In most cases, this abnormality is only anatomical and there are no symptoms. On the other hand, in others it can produce pain due to subacromial shock or instability in the aberrant area.
Impingement of the muscles can occur for various causes, the main ones being: trauma, microtrauma, degenerative problems, morphology or inclination of the acromion, tenosynovitis of the long head of the biceps, thickening of the coracoacromial ligament, instability of the glenohumeral joint, among others..
A common cause of rotator cuff impingement is the acromial spur or osteophyte. The acromial spur is a bone lump or tumor that generally occurs on the lower and anterior aspect of the acromion. It is caused by degenerative changes in which abnormal bone proliferation occurs at that point.
Impingement syndrome occurs in stages, going from less to more. The bursa or synovial bag is a loose connective tissue that serves as a lubricant for the joint during movements, separating muscles and bones, preventing them from directly touching (friction or shear). When the harmony of the shoulder joint is lost, the impingement process can begin.
The first step of this injury (stage I) is the development of a bursitis or tendonitis, called subacromial bursitis or impaction syndrome. In bursitis, the connective tissue is inflamed and if this persists the tendons and muscles also become inflamed..
Stage II is tendinosis, where the tendons begin to wear down, degenerate, and weaken. In stage III the rotator cuff tendons are partially or totally ruptured.
The treatment for this pathology is subacromial decompression, this is a surgical procedure, which can be performed arthroscopically..
This procedure involves removing the inflamed tissue, the coracoacromial ligament, and part of the acromion bone to make it square (achromoplasty). In this way, the subacromial space is increased and friction of the rotator cuff tendons with the acromion bone is avoided..
The union of the clavicle with the acromion can suffer trauma that injures this union to different degrees. Injuries are classified into 3 grades.
In first-degree dislocation, the trauma is mild and there is only a stretch of the acromioclavicular ligament.
While, in the 2nd degree there is a slight tear of both the acromioclavicular and coracoclavicular ligaments. Finally, the 3rd degree both ligaments are completely torn.
This pathology is characterized by the degeneration of the cartilage of the acromioclavicular joint due to aging or excessive movement of the shoulder. There may be hypertrophy of the joint, inflammation, and formation of osteophytes that generate spiny projections on the bone. All this generates joint pain.



Yet No Comments