The pulseless electrical activity (AESP) it is a mechanical heart failure in which there is electrical activity of the heart, but there is no effective contraction and cardiac output falls. In other words, as no effective contraction occurs, there is no blood flow.
It is a very serious pathological situation that, even under hospital care, has a high mortality rate. However, immediate treatment aimed at correcting the cause of pulseless electrical activity (PSA) can lead to rapid and sustained recovery..
Pulseless electrical activity occurs in approximately 30% of patients with cardiac arrest. The survival rate of these patients is much worse than those with shockable rhythms.
Many studies suggest that treatment for the specific cause of PSA is much more effective than advanced cardiac life support with cardiac massage, epinephrine, and vasopressin. In fact, it could be added that high doses of epinephrine have been associated with worse results..
Pulseless electrical activity is an emergency situation that requires highly trained personnel to handle and resolve. Patients who present with AESP outside the hospital have a much worse prognosis than those who are within a hospital service.
The American and European societies of ACLS (Advanced Cardiac Life Support or Advanced Cardiac Life Support) have emphasized the need for a rapid diagnosis of the cause of AESP to apply timely and immediate treatment and to save the life of the patient.
Article index
The general signs of AESP are collapse and loss of consciousness (unconsciousness), agonal breathing or apnea (absence of respiration), and absence of a pulse detectable by arterial palpation..
Some authors believe that the classification of entities that can occur with PSA, grouped with the letters H and T to facilitate memory, are very extensive and make a differential diagnosis in the few minutes available to provide timely treatment is hard. The list is included below.
However, some authors have published simple classifications based on some electrocardiographic signs that are discussed below.
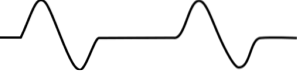
In the electrocardiographic recording of these patients, there is electrical activity, that is, the waves that correspond to the electrical activity of the atria and ventricles are recorded..
When registering the QRS complex (ventricular electrical activity), it is observed that there are two types of registration in these patients. One with narrow QRS complexes with times less than 0.12 seconds, and another with wide or wide QRS complexes with a duration greater than or equal to 0.12 seconds.
These electrocardiographic signs allow to direct the diagnosis, since the narrow QRS complexes are associated with mechanical problems caused by obstructions of the entrance or exit of the right ventricle.
Wide QRS complexes are associated with metabolic problems or with ischemic failure (failure of oxygen delivery to myocardial tissue) of the left ventricle.
The four most common mechanical causes of cardiac arrest with pulseless electrical activity are cardiac tamponade, tension pneumothorax, mechanical hyperinflation, and pulmonary embolism..
In these cases, jugular distention and dull or muffled heart sounds suggest cardiac tamponade. Rib fractures, emphysema, positive pressure ventilation, and chest hyperexpansion suggest tension pneumothorax or mechanical hyperinflation.
History of cancer or deep vein thrombosis suggests pulmonary embolism. Cardiac tamponade can also be caused by a myocardial rupture in the course of infarction..
A collapsed right ventricle suggests admission problems due to cardiac tamponade, pneumothorax, or hyperinflation. A dilated right ventricle may indicate a pulmonary embolism. In these cases, a chest ultrasound can help evaluate the pleura and diagnose pneumothorax..
Wide QRS complexes are associated with severe metabolic problems such as hyperkalemia with or without acidosis and toxins that block sodium channels.
In patients with critical illnesses such as sepsis, shock or renal failure, the presence of wide QRS complexes is usually associated with hyperkalemia. The presence of an arteriovenous fistula or a dialysis catheter is also more frequently associated with hyperkalemia.
Patients with a suicide attempt due to ingestion of a substance and who are admitted with EPA imply that, in most cases, the poison ingested is a substance that blocks sodium channels.
Metabolic or ischemic causes have an electrocardiographic support and can be easily diagnosed.
Ischemic causes such as myocardial infarction, when they affect large areas of the left ventricle, may be accompanied by mechanical failure of the left ventricle and are, in this case, the cause of pulseless electrical activity.
There is a list of eleven conditions that can occur with pulseless electrical activity and which have been arranged with the initial letters H and T for ease of memory (as a mnemonic) and these are:
Hipovolaemia (decreased volume of circulating blood).
Hipoxia (decreased blood and / or tissue oxygen).
Hydrogen ion - acidosis (increased plasma concentration of hydrogen ions).
Hiperkalemia (increased potassium in the blood).
Hipokalemia (decreased potassium in the blood).
Hipothermia (decrease in body temperature).
Toxines.
Tcardiac aponation (increased fluid, blood, or gas around the heart that compresses it and blocks its mechanical function).
TPTX ension (tension pneumothorax presence of tension air in the mediastinum that compresses and displaces all the viscera including the heart and large vessels such as the aorta).
Tcoronary rhombosis (thrombi in one of the coronary arteries that impede the blood flow that nourishes the heart muscle).
Tpulmonary rhombosis (thrombi in the pulmonary circulation).
In patients in whom a mechanical etiology of pulseless electrical activity with narrow QRS complexes is suspected, treatment is initiated with aggressive administration of fluids or fluids..
Then, based on the clinical, electrocardiographic and bed ultrasound data, we proceed to pericardiocentesis (extraction of the pericardial fluid) in case of cardiac tamponade; to needle puncture for chest decompression in case of tension pneumothorax and to adjustment of ventilation or thrombolytic therapy.
When the QRS complexes are wide and hyperkalemia is suspected, calcium chloride and bicarbonate are given. In the case of sodium channel blockers, intravenous boluses of sodium bicarbonate are administered..
Although this classification simplifies diagnosis and helps to direct therapy more efficiently, it has its limitations. However, it is still a practical classification for immediate emergency action to safeguard the life of the patient..

Yet No Comments