The craniosynostosis It is a rare problem of the skull that causes the baby to develop or present deformations in the head at birth. It is about the early fusion of the different parts of the skull so that it cannot grow properly, interrupting the normal development of both the brain and the skull..
In the newborn, the skull is made up of several bones that are not joined yet, this is so that the brain has enough space so that it can continue to develop. In fact, the bones of the skull will double in size during the first three months of life and do not fully fuse until the late teens..

In reality, the level of fusion of the skull bones changes with age and depending on the sutures; closing some before others. The newborn's skull is made up of seven bones, and they develop through two processes: bone displacement and bone remodeling..
It seems that the skull consists of a single compact piece, however, contrary to what you may think, the skull is more like a soccer ball: it has a series of bones arranged in plates that fit together, building a sphere..
Between these plates are strong elastic tissues called sutures. These are what give the skull the flexibility to develop as the brain grows. This flexibility also allows the baby to be delivered through the birth canal..
What happens is that when an area of the skull that is growing fuses and closes, other areas will try to compensate for this, becoming more prominent and altering the normal shape of the head..
Craniosynostosis can also appear in the literature as synostosis or premature closure of sutures.
Article index
There are several types of craniosynostosis depending on the parts of the skull that are altered and the resulting shape of the head..
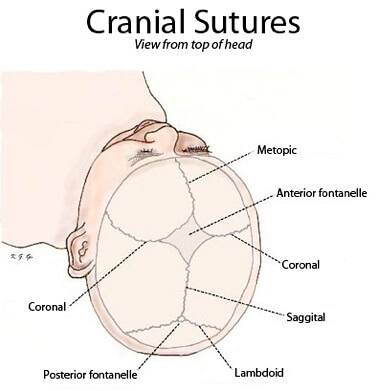
It is the most common type and affects men most often. It is the premature fusion of the sagittal suture, which is located in the midline of the upper part of the skull and goes from the soft point (also called fontanel) to the back of the head.
It results in a long and narrow head shape. As it grows, the back of the head becomes more prominent and pointed, and the forehead protrudes. This type is the one that poses the least problem for normal brain development and is relatively easy to diagnose.
It consists of the early union of one of the coronal sutures, where the forehead and frontal lobe of the brain grow forward. In this type, the forehead appears flattened, and the eye sockets raised and sloping.
In addition, these protrude and the nose is also deviated to one side. A sign that the baby has this type of craniosynostosis is that he will tilt his head to one side to avoid seeing double..
It is the junction of the metopic suture, which is located in the middle of the forehead of the affected person and goes from the soft point or fontanelle to the beginning of the nose.
It causes the eye sockets to come together and the eyes are very close to each other. The forehead takes a protruding triangular shape.
It is the least common, and results from a premature closure of one of the lamboid sutures that are in the back of the head.
This results in a flattening of this area of the skull, making the bone behind the ear (mastoid bone) protrude, which is manifested in one ear lower than the other. In this case, the skull may also be tilted to one side..
All these correspond to unions of a single suture, but there may also be unions of more than one.
For example:
- Anterior brachycephaly: it is called bicoronal, as it occurs when the two coronal sutures, which go from ear to ear, fuse prematurely, presenting the forehead and eyebrows area flat. The skull in general looks wider than normal.
- Posterior brachycephaly: the skull also widens, but due to the union of the both lamboid sutures (which, as we said, are in the back).
- Scaphocephaly of the satigal suture and the metopic: the head has an elongated and narrowed appearance.
For example:
- Turribrachycephaly, by the union of bicoronal, sagittal and metopic sutures: the head is pointed, and is characteristic of Apert syndrome.
- Multisutures joined that give the skull a "clover leaf" shape.
This disease is rare, affecting about 1 in 1,800 to 3,000 children. It is more common in men, with 3 out of 4 male cases being affected, although this seems to vary depending on the type of craniosynostosis..
Between 80% and 95% of cases belong to the non-syndromic form, that is, as an isolated condition, although other authors have estimated that between 15% and 40% of patients may be part of another syndrome.
Regarding the types of craniosynostosis, it seems that the most frequent is the one that involves the sagittal suture (40-60% of cases), followed by the coronal (20-30%) and, then the metopic (10% or less). The union of the lambdoid suture is very rare.
Craniosynostosis can be syndromic, that is, it is linked to other rare syndromes. A syndrome is a series of associated symptoms that arise from the same cause and that in most cases it is usually genetic.
What is known as secondary craniosynostosis can also occur, which is more common, and which has its origin in a failure in brain development.
Usually it will lead to microcephaly or reduced cranial size. Therefore, here craniosynostosis will appear together with other problems of brain development such as holoprosencephaly or encephalocele..
It can also be caused by teratogenic agents, this means any chemical substance, deficiency state or some harmful physical agent that produces morphological alterations in the fetal stage. Some examples are substances such as aminopterin, valproate, fluconazole or cyclophosphamide, among others..
- On the other hand, it can also be non-syndromic; the causes being variable and not fully known.
It is known that there are factors that can facilitate craniosynostosis such as:
- Little space within the uterus or abnormal shape of the uterus, mainly causing coronal synostosis.
- Disorders that affect bone metabolism: hypercalcemia or rickets.
- It can sometimes be due to hematological (blood) disorders, such as congenital hemolytic jaundice, sickle cell anemia, or thalassemia.
- In some cases, craniosynostosis is a consequence of iatrogenic problems (that is, caused by the error of a doctor or health professional)
In some cases, craniosynostosis may not be noticeable until a few months after birth. Specifically, when it is associated with other craniofacial problems, it can be seen from birth, but if it is milder or has other causes, it will be observed as the child grows.
In addition, some symptoms described here usually appear in childhood..
- The fundamental one is the irregular shape of the skull, which is determined by the type of craniosynostosis it has..
- A hard ridge can be felt to the touch at the suture junction area.
- The soft part of the skull (fontanel) is not noticeable or is different than normal.
- The baby's head does not seem to grow in proportion to the rest of the body.
- There can be an increase in intracranial pressure that can occur in any type of craniosynostosis. It is obviously due to malformations of the skull, and the more sutures that are attached, the more common this increase will be and the more serious it is. For example, in the type of multiple sutures, an increase in intracranial pressure will occur in approximately 60% of the cases, while in the cases of a single suture the percentage decreases to 15%..
As a consequence of the previous point, the following symptoms will also occur in craniosynostosis:
- Persistent headache, mainly in the morning and at night.
- Vision difficulties such as seeing double or blurry.
- In slightly older children, decreased academic performance.
- Delayed neurodevelopment.
- If increased intracranial pressure is not treated, vomiting, irritability, slow reaction, swelling of the eyes, difficulty in following an object with sight, hearing and breathing problems may occur.
Importantly, not all skull deformities are craniosynostosis. For example, an abnormal head shape may occur if the baby stays in the same position for a long time, such as lying on the back..
In any case, it is necessary to consult a doctor if it is observed that the baby's head is not developing properly or has irregularities. However, the diagnosis is favored since routine pediatric check-ups are made to all babies in which the specialist examines the growth of the skull.
If it is a milder form, it may not be detected until the child grows older and there are increases in intracranial pressure. Therefore, the symptoms indicated above should not be ignored, which in this case would appear between 4 and 8 years of age..
The diagnosis should include:
- A physical exam: palpating the head of the affected person to check if there are ridges in the sutures or to observe if there are facial deformities.
- Imaging studies, such as computed tomography (CT), which will allow you to see the sutures that have been attached. They can be identified and it is going to observe that where there should be a suture there is not one, or else, that the line protrudes in a crest.
- X-rays: to obtain accurate measurements of the skull (via cephalometry).
- Genetic testing: if it is suspected that it may be of a hereditary type linked to a syndrome, with the aim of detecting which syndrome would be and treating it as soon as possible. They usually require a blood test, although sometimes samples of other tissues such as skin, cells from the inside of the cheek, or hair can also be tested..
There are more than 180 different syndromes that can cause craniosynostosis, although all of them are very rare. Some of the most distinctive are:
- Crouzon syndrome: this is the most common and is associated with bilateral coronal craniosynostosis, midface abnormalities, and bulging eyes. It appears to be due to a mutation in the FGFR2 gene, although some cases arise spontaneously.
- Apert syndrome: He also has bilateral coronal craniosynostosis, although other forms of synostosis can be seen. There are fusions at the base of the skull, in addition to deformities in the hands, elbows, hips, and knees. Its origin is hereditary and gives rise to characteristic facial features.
- Carpenter syndrome: This syndrome is usually associated with posterior plagiocephaly or union of lamboid sutures, although scaphocephaly also appears. It is differentiated by deformations also in the extremities and by one more digit in the feet, among other things.
- Pfeiffer syndrome: Unicoronal craniosynostosis is common in this condition, as well as facial deformities, which cause hearing problems, and in the extremities. It is also associated with hydrocephalus.
- Saethre-Chotzen syndrome: they usually present with craniosynostosis of the unilateral coronal type, with very limited development of the anterior cranial base, very low hair growth, facial asymmetry, and delayed development. It is also of the congenital type.
Efforts should be made to develop early treatment, as many of the problems can be fixed by the rapid growth of the brain and the flexibility of the baby's skull to adapt to changes..
Even in very mild cases, no specific treatment may be recommended, but its cosmetic effects are expected to be less severe as the affected person develops and grows hair..
If the cases are not very serious, it is advisable to use non-surgical methods. Normally, these treatments will prevent the progression of the disease or they will improve, but it is usual that there continues to be a certain degree of disfigurement that can be solved with simple surgery.
If we are in a situation in which there have been other deformations in the skull such as positional plagiocephaly, or a flattened side of the head due to being in the same position for a long time, due to pressure from the uterus or complications in childbirth, we can return to normal head shape with a custom shaping helmet for baby.
Another option is repositioning, which has been effective in 80% of cases. It consists of placing the baby on the unaffected side, and working the neck muscles by placing him face-down, on his abdomen. This technique is effective if the baby is less than 3 or 4 months old..
Surgical intervention carried out by a craniofacial surgeon and a neurosurgeon is indicated in cases of serious craniofacial problems, such as lamboid or coronal craniosynostosis, or if there is an increase in intracranial pressure.
Surgery is the treatment of choice for most craniofacial malformations, especially those associated with a major syndrome.
The goal of the surgery is to decrease the pressure that the skull is putting on the brain and to provide enough space for the brain to grow, as well as to improve physical appearance..
After surgery, you may need a second intervention later if you tend to develop craniosynostosis as you grow older. The same happens if they also have facial deformities.
Another type of surgery is endoscopic, which is much less invasive; since it involves the introduction of an illuminated tube (endoscope) through small incisions in the scalp, to detect the exact location of the fused suture to open it later. This type of surgery can be done in as little as one hour, the swelling is not as severe, there is less blood loss, and recovery is faster..
In the case of other underlying syndromes, periodic monitoring of skull growth is necessary to monitor the appearance of increased intracranial pressure..
If your baby has an underlying syndrome, the doctor may recommend regular follow-up visits after surgery to monitor head growth and check for increased intracranial pressure..


Yet No Comments