The Leopold maneuvers they are part of the prenatal clinical examination that, through abdominal palpation, determines the fetal position in the maternal uterus. This technique consists of four steps or maneuvers that provide information on the fetal presentation, situation, attitude and position..
The development of this procedure is due to the German physician Christian Gerhard Leopold (1846-1911). Leopold was a surgeon, gynecologist, and obstetrician with an interest in the thorough clinical evaluation of pregnant women. This interest led him to establish in 1894 the four steps of the procedure that today bears his name..
Leopold maneuvers are part of the prenatal evaluation, along with the pelvic examination and fetal well-being. Correct execution of the examination steps provides data on intrauterine fetal statics, in addition to providing the estimated weight of the fetus. The presence of dystocia may also be evident.
Dystocia designates the incorrect position of the fetus within the uterus that prevents the development of natural childbirth. By determining the fetal position, a normal delivery or the need for a cesarean section can be predicted. For this reason, the correct execution of the Leopold maneuvers is important in routine prenatal care..
Article index
The procedure developed by Leopold was designed to determine intrauterine fetal statics. In addition, data regarding fetal weight and amount of amniotic fluid can be obtained..
Leopold's maneuvers can be performed from 32 weeks of gestation, has few limitations and no contraindications.
Fetal statics is the spatial relationship that the fetus maintains with respect to the maternal uterus and pelvis. Parameters such as fetal position, presentation, attitude and position can be distinguished.
It is the correspondence between the longitudinal axes of the fetus and the mother. The most frequent situation is longitudinal and facilitates labor.
The transverse and oblique situations are transitory, but their persistence towards the end of gestation indicates the possibility of a cesarean section..
It corresponds to the fetal structure that is in relation to the pelvis and that, by occupying it, can initiate labor. A fetus in longitudinal position will have a cephalic presentation the vast majority of the time.
The less frequent abnormal presentations are breech, hip, face or hand presentation. Shoulder presentation is rare, and is related to a transverse situation.
It is determined by the position of the parts of the fetus and the relationship between them. The fetal attitude can be in flexion, indifferent, extension or hyperextension.
This attitude varies throughout the gestation, but at the end of it it already adopts its definitive attitude. An attitude in flexion is more frequent and allows a labor without difficulties.
The fetal back is usually taken as a reference to define its position. The back can be on the right or left, which is the most common. A forward or backward back is very rare.
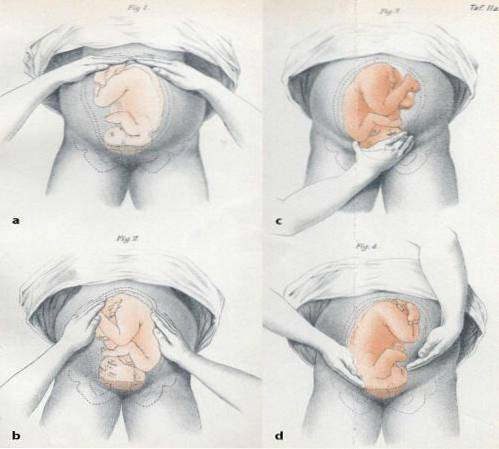
The evaluation is bimanual and it is about locating the fetal pole located in the uterine fundus. The doctor's or nurse's hands should be located on the patient's upper abdomen. Gentle palpation of the fundus determines which fetal pole is there.
The cephalic pole is rounded and hard, while the breech location is usually irregular. The irregularity that appears to be palpating nodules may show a breech presentation.
It is the bimanual palpation of the sides or paraumbilical surfaces to locate the position of the fetal dorsum. In this phase it is palpated gently, firmly and deeply, in order to find the fetal spine.
The spine is hard and slightly arched, and can be easily delimited. The extremities are palpable as small mobile structures.
The third maneuver is performed by palpating the suprapubic region with the fingers of the dominant hand. The objective is to determine the fetal pole that is located at this level, as well as the progress of labor.
A fixed structure over the pubis suggests the embedding of the fetal pole in the maternal pelvis. A movable pole will indicate an empty pelvis. Through this maneuver it is also possible to obtain data to estimate fetal weight.
It is a bimanual palpation that is performed by placing the hands on each side of the lower hemiabdomen. The intention is to know the fetal pole in relation to the maternal pelvis. The doctor is looking at the feet of the patient, and with the tips of the fingers pushes in the direction of the pelvis.
The cephalic pole is easily delimited, evidenced by the separation or divergence of the fingers of the hands.
One of the advantages of performing the Leopold maneuvers is being able to obtain data to estimate fetal weight. This is achieved by the Johnson Toshach method or formula created in 1954, before the advent of ultrasound..
Both the measurement of the uterine height and the position of the fetal pole with respect to the pelvis (third maneuver) are useful to perform the calculation. When the presentation is above the pelvis, the calculation is made with the formula:
PF = (AU - 12) X 155
If the presentation is at pelvic level or embedded, the formula will have a slight variation:
PF = (AU - 11) X 155
Sometimes the estimation of fetal weight by the Johnson-Toshach method is usually more accurate than measurements made by ultrasound..
Each physical examination technique has characteristics that distinguish it, such as its usefulness, ease, and advantage over other techniques..
The Leopold maneuvers are a reflection of simplicity, practicality and the data they provide to the prenatal examination are useful. The advantages of this procedure are:
- Ease of realization.
- They are not invasive.
- Minimum requirements.
- Does not require instruments.
- They are inexpensive.
- It is a painless technique.
- The training to perform them is fast.
- Useful when ultrasound is not available, but is not a substitute for it.
- The results are usually reliable.
- Its use is universal and without contraindications.
- It allows to know which intervention is more appropriate, childbirth or cesarean section.
The limitations for executing the Leopold maneuvers are few, which is an additional advantage. It is a simple, non-invasive and painless technique, provided it is well executed. However, there are conditions that limit the obtaining of reliable data when performing them:
- Low examiner skill.
- Very small fetuses.
- The onset of labor, as it is often painful.
- Apprehensive or low pain threshold patients.
- Lack of knowledge on the part of the patient or the examiner of its usefulness.

Yet No Comments