The rhomboid major and minor muscles They are superficial muscles located in the upper posterior part of the trunk (back). Its nomenclature comes from Latin musculus rhomboideus major Y musculus rhomboideus minor.
Both muscles are closely located, with a small gap between them, although there are points on their bordering margins where they join. These muscles are twinned by their great similarity in terms of shape, location and function, hence they have the same name, differing only by the volume they occupy..
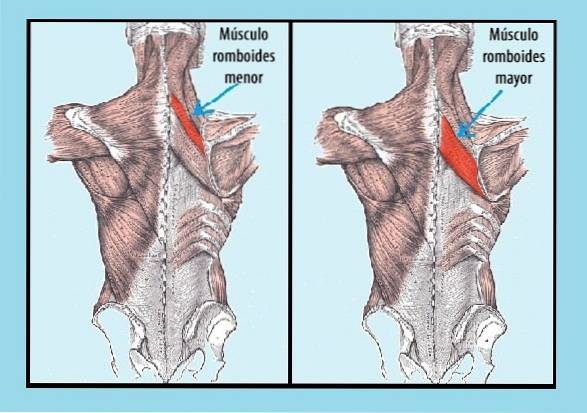
The rhomboid minor, is smaller in size and is located in the upper part. While the rhomboid major has larger dimensions and is located below the rhomboid minor. For this reason, some authors call the minor and major rhomboids superior and inferior rhomboids respectively..
Regarding the functions that these two muscles fulfill, it can be said that they are synergistic, they act together for the same objective, since both collaborate in two very important movements of the scapula.
The movements are adduction, which means that the scapula is closer to the medial line of the spine and in the lifting movement of the scapula.
Article index
As has been mentioned, the rhomboids minor muscle is also called the superior rhomboids, since it is located before the rhomboids major. For this reason, the greater rhomboids are known as inferior rhomboids, as they are immediately after the minor rhomboids.
The rhomboid major and minor muscles, despite being located below the trapezius, belong to the group of superficial muscles of the back. They are paired muscles that are found on each side of the back symmetrically..
The muscles are flattened and, as the name suggests, are diamond-shaped. That is, they have 4 sides and their vertices have unequal angles (two acute and two obtuse).
The rhomboid minor is inferior to the levator scapulae. It is a relatively small and thin muscle compared to the rhomboid major. Whereas, the rhomboid major is large and broad compared to the rhomboid minor and abuts the latissimus dorsi muscle in its lower part.
They are born in the spinous processes corresponding to the cervical and thoracic vertebrae, depending on the muscle.
The rhomboid minor originates from the supraspinatus ligaments of the processes of the C7 and T1 vertebrae, while the rhomboid major arises from the same ligament but from the spinous processes of the thoracic vertebrae T2 to T5.
Its fibers descend transversely from its point of origin to its insertion site.
The rhomboid minor joins at the medial and posterior border of the shoulder blade (opposite the root of the spine of the scapula), specifically at the upper end of the shoulder blade, shortly before it joins the spine. Its insertion site precedes the site where the fibers of the greater or lower rhomboid attach.
The rhomboid major is inserted into the scapula just after the fibers of the rhomboid minor muscle end, that is, on its medial edge of the scapular dorsum, touching a large part of its surface, until reaching the inferior angle.
The dorsal nerve of the scapula (C4-C5) is in charge of innervating both the rhomboid minor or superior muscle, and the rhomboid major or inferior muscle. This nerve comes from the brachial plexus.
The rhomboid major muscle is supplied by branches from the transverse cervical artery.
Both muscles collaborate in the union of the spine with the scapula. That is why they have an influence on the movement of the scapula and its fixation to the chest wall, that is, it gives it stability..
The contraction of these muscles generates a backward movement of the scapula, bringing the scapula closer to the spine, with some internal and lower belling (scapular adduction or retraction movement).
This movement is done in collaboration with the middle part of the trapezius. Whereas, the serratus anterior muscle opposes (antagonist).
On the other hand, the lifting movement of the scapula is accompanied by other muscles that act synergistically with the rhomboids, these are: the levator scapulae and upper part of the trapezius.
The functions of the rhomboid muscles are revealed in the warrior posture (arms crossed) and also in the slant plank position..
One of the effects that the rhomboid muscles could suffer is their lengthening or weakness, although this is not frequent. If these muscles are lengthened, the normal alignment of the scapula is lost..
Trigger points (painful knots of muscle contracture) in the rhomboids can appear as a consequence of a tightness of the major and minor pectoral muscles. This produces traction on the rhomboids.
Therefore, if you plan to do rehabilitation and exercises for the rhomboid muscles, you should also think about restoring the pectoral muscles, regardless of whether or not there is pain referred to them..
Patients with trigger points in the rhomboids complain of pain around the shoulder blade.
The pain is accentuated if the arm is stretched forward to reach something with the hand. On the other hand, the movement of the shoulder blade can produce noise, click type.
If shoulders loaded forward are observed, suspect joint involvement with the pectorals.
This syndrome is mainly caused by poor postural hygiene, triggering a series of alterations in the anterior and posterior muscles of the trunk. In some, muscle tone is increased while in others it creates weakness and flaccidity..
Other causes can be congenital morphological asymmetries, poorly guided training, poorly executed exercises, postures taken for a long time with head and shoulders advanced in relation to the body. A clear example is reading on a computer screen for several hours.
This position generates excess tension in the muscles of the cervico-cranial area, causing headaches and neck pain..
In this syndrome, the pectoralis major, pectoralis minor, upper trapezius, sternocleidomastoid, and levator scapulae muscles may be hypertensive..
While, the major and minor rhomboids can be strongly weakened, as well as other muscles such as: serratus anterior or middle and lower trapezius, among others..
This situation produces instability of the scapula and, as a consequence, an alata or winged scapula can be originated.
This anomaly presents with hyperextension of the head, with thoracic kyphosis and drooping shoulders. There is weakness in the deep flexor muscles of the neck, rhomboids and serratus anterior. While the pectoral muscles (major and minor), upper trapezius and levator scapulae are retracted.
The head in a forward position favors or predisposes the impingement of the dorsal nerve of the scapula. This produces gradual weakness of the angular muscle of the scapula and the rhomboid muscles..
This situation results in shoulder protraction and internal rotation of the humerus as compensation..
It is possible to know if there is weakening of the rhomboid muscles, if fatigue appears when trying to keep the arms open.
On the other hand, it can be palpated. To do this, the patient is placed on his stomach and helps to position the back of the hand towards the back, also serving to lift the arm upwards. Both positions allow the examiner to touch the edge of the shoulder blade and thus locate these muscles..
Once located, gentle massages can be done from the inside out and from the top down, this in order to stretch the muscle. It culminates by pressing in a circle.
Another way to explore it is with the patient face down and the arm stretched out with the elbow flexed. The patient is asked to retract the shoulder blade bone (medial glide) while the examiner resists, putting pressure on the bone itself.
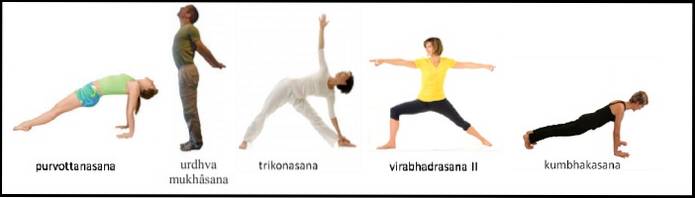
The exercises or positions recommended to strengthen these muscles are the following:
- Purvotanasan, urdhva mukhâsana (these pull the shoulders back).
- Trikonasana, virabhadrasana II (positions that involve opening your arms).
- Kumbhakasana (fixes the shoulder blade to the ribs). See the following figure.
On the other hand, there are exercises or positions that help to make these muscles more flexible or stretch, these are: garudasana, ardha matsyendrasana, balasana. See next figure.

The patient can lie on his back and cross one arm to the opposite side to stretch the shoulder blade outward. Then place a tennis ball on the edge of the shoulder blade and apply pressure along the entire edge, letting the ball slide (preferably up and down).



Yet No Comments