
Broca's aphasia is undoubtedly one of the best known. The study of aphasias began to be studied in 1861 by Paul Broca (1924-1980), although he called them aphasia. The term aphasia was not introduced until 1884 by Armand Trousseau (1801-1867). But what is an aphasia? It is a pathological state in which language is altered as a result of a brain injury.
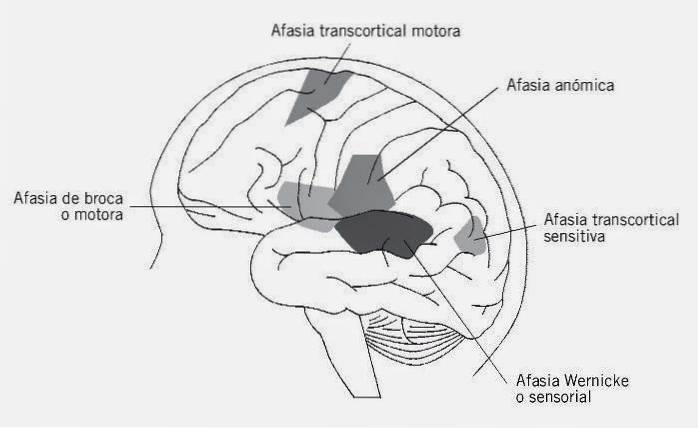
There are different types: Broca's, Wernicke's, conductive, global aphasia, etc. Each of them with different characteristics but with a common element, the alteration of language. Throughout this article we will delve into Broca's Aphasia.
Contents
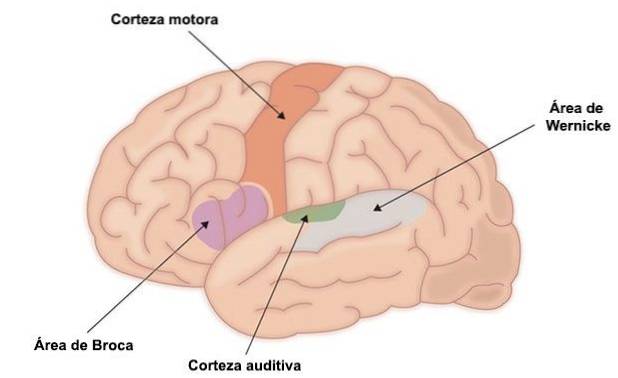
The most frequent causes are strokes in the area of the left middle cerebral artery. It is an artery that irrigates the language areas, therefore, when it is affected, it has a direct impact on language. Other causes can also be brain tumors, infections, surgery or traumatic brain damage..
Lesions limited to Broca's area (Brodmann's areas 44 and 45) are not sufficient to produce aphasia itself. In this case, slight defects in the agility of articulation, a certain "foreign accent" and a reduction in the ability to find words are observed. Hemiparesis and apraxia are usually minimal. It is a restricted form of Broca's aphasia that is called type I, minor or Bronca Area Aphasia..
"Language is the dress of thoughts." -Samuel Johnson-
Broca's aphasia in its extensive form is seen if the damage extends to the opercular region, the anterior insult, the precentral gyrus, and the paraventricular and periventricular white matter. It is called extended or type II.
There is a lack of fluidity. Their communication is based on the use of single words and short phrases produced with slowness, difficulty and great effort. Phonological paraphasias are observed due to errors in phoneme selection. Omissions and simplifications of consonant groups also tend to appear frequently (González and González, 2012).
Dysarthria is also usually appreciated, that is, problems in the motor execution of speech, so that all of the above can be worsened. Ungrammatical expression is another symptom of Broca's aphasia. This causes the appearance of agrammatism, which is defined as "the difficulty of the patient to use correct constructions from the morphosyntactic point of view (Arnedo, Bembibre and Triviño, 2012)".
"The limits of my language are the limits of my mind." -Ludwig Wittgenstein-
Nor does the use of functional terms such as "a", "he", "some" ... Just as grammatical or auxiliary markers are not usually appreciated. Frustration and helplessness can be seen on the part of these patients who try to speak but find it very costly to be able to express themselves normally.
Anomia is also another characteristic of patients with Broca's aphasia, in fact, it is one of the primary symptoms. Anomie refers to the difficulty in finding the correct word from the alteration that occurs in the ability to select the specific programs of each individual word.
The naming is usually poor, although it is usually improved if the patient is supported with contextual and phonetic aids.
Reading in this type of patient is slow, choppy and performed with great difficulty. Reading aloud is quite impaired and compression is similar to oral.
The writing is altered. Spelling errors such as spelling omissions and substitutions occur. Motor and aphasic agraphia is shown.
The impaired comprehension is attributed to a deficit in syntactic processing. In reversible passive sentences, comprehension difficulties are also observed. Arnedo, Bembibre and Triviño (2012) emphasize that "the ungrammaticality in the production that accompanies Broca's aphasia seems to alter the ability of patients to use, in turn, said grammatical information in comprehension, such as the action of a computer series of words to decode the meaning of the phrase ".
An example of a neuropsychological evaluation of Broca's aphasia can be the following (Arnedo, Bembibre and Triviño, 2012):
As the brain recovers, there is a rapid restoration, which is known as spontaneous recovery. This recovery is explained by two causes: brain plasticity and repair of damaged tissue. Basso (2003) proposes that this phase can last between one and six months.
Traumatic aphasias have a better prognosis than vascular ones for several reasons:
According to Martinell (2011), the treatment of a patient with aphasia is an integrated set of interventions that are aimed at:
Junqué and his team (2004) propose that the intervention in patients with this type of aphasia should be the following objectives:


Yet No Comments