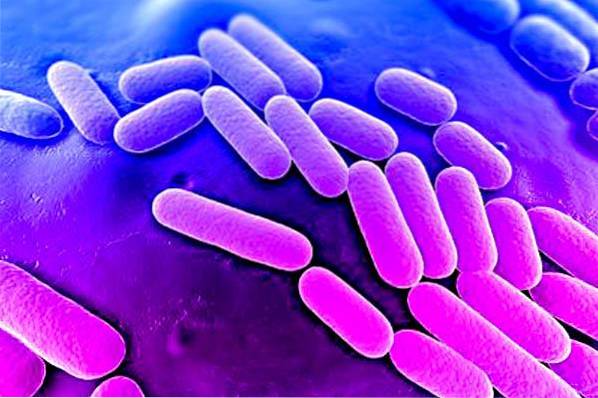
Klebsiella pneumoniae It is a facultative, Gram negative, anaerobic bacterium that does not produce spores and is in the form of a bacillus. It belongs to the group of coliforms, common bacteria of the gastrointestinal flora of humans and other vertebrates..
They are medically important because they are opportunistic (that is, they take advantage of a weakened immune system), and can cause disease.
Klebsiella pneumoniae it is an important bacterial agent, capable of causing infectious diseases in human populations. It is also one of the main causative agents of hospital-acquired infections of bacterial origin, especially in patients with weakened immune systems. It is responsible for respiratory and urinary infections, pneumonia, among others.
Article index
Bacteria of the genus Klebsiella belong to the Enterobacteriaceae family that are characterized, among other aspects, because they are Gram negative bacilli that do not have movement.
Another characteristic that differentiates them from the rest of the Enterobacteriaceae is that the outermost cell layer is formed by a capsule of polysaccharides. In addition to K. pneumoniae, andThe genus is made up of other species such as K. terrigena, K. oxytoca Y K. planticola.
Klebsiella pneumoniae Lactose ferments with gas formation in 48 hours. This species can develop in the presence or absence of free oxygen, which is why it is considered a facultative anaerobic species. It can survive in alkaline pH but not in acidic pH, the optimal development occurs in a medium with neutral pH.
Its development temperature is between 15 and 40 ° C, however in laboratories the strains are cultivated at 37 ° C. It has beta-lactamase enzymes. The surrounding capsule increases its virulence by acting as a physical barrier to evade the host's immune response. This capsule also protects the cell from desiccation..
Klebsiella pneumoniae it is a microorganism typical of the microbiota of humans and other vertebrates. It can be found in the mouth, skin, and intestinal tract, where it does not initially cause infectious problems..
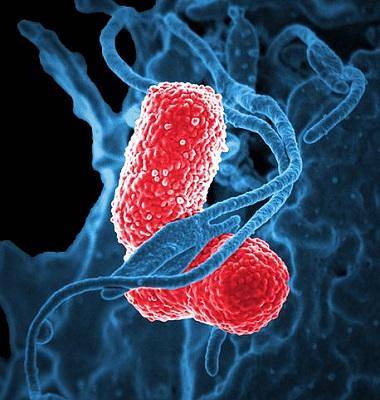
Klebsiella pneumoniae It is shaped like a cane. It is short, measuring between 1 - 2 by 0.5 - 0.8 micrometers. Cells can be found individually, in pairs, in chains, and sometimes in groups. It does not present a flagellum (so it is not mobile) and has a prominent capsule.
The bacteria K. pneumoniae develops a large colony of mucoid consistency when grown on primary isolation medium, on Mac Conkey agar and on Blood Agar. The polysaccharide capsule is responsible for the mucoid appearance of the colony of K. pneumoniae.
Klebsiella pneumoniae it is an opportunistic pathogen that commonly causes nosocomial infections. In recent years, hypervirulent strains (mainly K1 and K2) increasingly affect previously healthy people, that is, they were not hospitalized patients.
The increase in virulence is due to increased production of polysaccharide capsules. Bacteremia by K. pneumoniae causes significant morbidity and mortality in general populations.
The abdominal cavity, the urinary tract and the lungs, in that order, are the sites most attacked by Klebsiella pneumoniae in people who have acquired the disease outside of hospitals.
This species is the second most common cause of infection by Gram negative bacteria after Escherichia coli. Certain underlying diseases can affect an individual's defenses and increase the risk of infection by K. pneumoniae. These diseases include cirrhosis, biliary tract disorders, diabetes mellitus, and alcoholism..
In the case of infections acquired in hospitals, colonization of the gastrointestinal tract by K. pneumoniae usually occurs before the development of infections.
Colonization by K. pneumonia it can also occur in the urinary tract, respiratory tract, and blood. Metastatic infections, such as pyogenic brain abscess, meningitis, and endophthalmitis, are the most important features of infections due to K. pneumoniae.
To get an infection by K. pneumoniae, the person must be exposed to the bacteria. Namely, K. pneumoniae must enter the respiratory tract or blood.
Direct transmission from the environment is unlikely. Biofilms from K. pneumoniae that are formed in medical devices (eg catheters and endotracheal tubes) provide one of the main means of infection in catheterized patients.
Klebsiella pneumoniae develops a polysaccharide capsule which is a determining factor in the pathogenicity of the bacteria. The capsule protects the microorganism from phagocytosis by polymorphonuclear cells.
Resistance to antimicrobial peptides and inhibition of dendritic cell maturation also play an important role in suppressing the early inflammatory response. Some capsular types are more virulent than others, such as types K1, K2, K4 and K5.
The first stage in infection is the adherence of the responsible agent to the host's cells. In Enterobacteriaceae, adherence is performed by the fimbriae or pilis. These fimbriae are another important virulence factor.
There are two main types of fimbriae, type 1 and type 3. Type 1 attach to cells in the main tubule of the urinary tract. Type 3 fimbriae allow adherence to endothelial cells and epithelial cells of the respiratory and urinary tracts.
Other additional virulence factors of K. pneumoniae include lipopolysaccharides, outer membrane proteins, as well as determining factors for the acquisition of iron and for the use of nitrogen sources.
Nosocomial infections caused by K. pneumoniae they tend to be chronic mainly due to their ability to form biofilms. These biofilms protect the pathogen from the host's immune system response as well as from antibiotics..
Another factor that helps K. pneumoniae becomes chronic is its resistance to multiple drugs. Resistance is commonly caused by the presence of extended-spectrum β-lactamases or carbapenemases, making it difficult to choose the appropriate antibiotics for treatment..
Klebsiella pneumoniae it can be treated with antibiotics if the infections are not resistant to the drugs. However, inadequate initial treatment is associated with increased mortality caused by the bacteria. Empirical antibiotic therapy can improve survival in patients with infections due to K. pneumoniae.
Combination therapies, effective in treating other resistant bacteria, are used cautiously to treat K. pneumoniae due to the potential for adverse events that may occur.
Combination therapies that include the use of aminoglycosides increase the risk of nephrotoxicity in the patient. Another possible severe adverse event is colitis associated with Clostridium difficile.
In recent years, several new antimicrobial agents with activity against strains of K. pneumoniae resistant to carbapenems, have advanced to Phase III clinical trials.
Ceftolozone, a new cephalosporin, in combination with tazobactam, has been effective in in vitro tests. Additionally, the development of new β-lactamase inhibitors, such as avibactam, and other new β-lactamase inhibitors and new generation aminoglycosides (neoglycosides), could help in the development of effective treatments against K. pneumoniae In the not too distant future.


Yet No Comments