
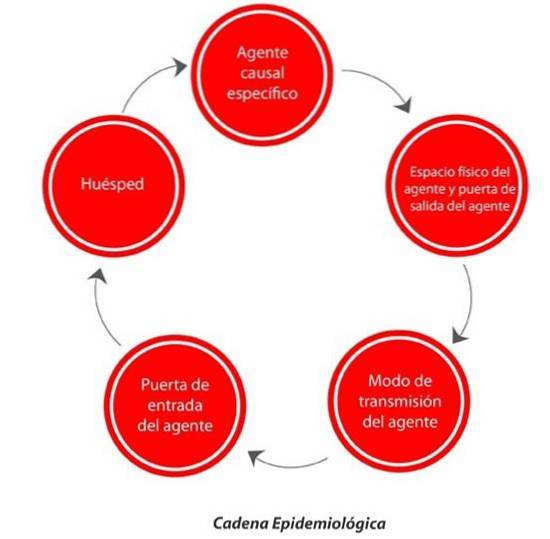
The epidemiological chain it is the result of the interaction of an agent, through a transmission route and a host, influenced by the environment.
The pathogenic agent, which is the one that starts the epidemiological chain, escapes from its reservoir and attacks another new host, infecting it in turn. It is considered that the environment influences the transmission of the pathogen, since the agent and the host are within it, as well as the route of transmission.
The study of an epidemiological chain is carried out with the objective of analyzing infectious diseases, identifying the links that make up the chain and preventing and controlling possible diseases. The use of prevention levels is proposed to prevent the epidemic from spreading in the population.
Some of these levels apply even before the pathological agent spreads, through the promotion of healthy lifestyle habits, such as good nutrition and physical exercise..
The pathological agent needs to be recognized before it is transmitted through the environment, thus preventing the spread of more hosts. For this reason, it is important to analyze the links in the chain and discover what the contagion point is..
If the chain is not stopped at its inception, it can trigger several unlimited epidemiological chains, turning the hosts into pathological agents and starting the chain from the beginning. You may also be interested in seeing epidemiological triad: definition and components.
The epidemiological chain begins with the causative agent, which is any pathogen that can cause disease. We can define a pathogen as bacteria or animal or plant toxins, necessary for the transmission of a disease.
The causative agent leaves the reservoir where it lives, through an exit door, to reach a new host. The reservoir is the natural habitat of the causative agent, on which it depends in order to survive and reproduce. The reservoirs can be animate (human), animal or inanimate (soil, fungi ...).
The carrier of the infectious agent is anyone who has the biological agent in their system, even if they do not present any symptoms or are eliminating it.
There are different types of carriers, they can be incubators, or convalescent. Incubators are those that may be infected by the pathogen without knowing it. Convalescents are carriers who are already suffering from the symptoms of the pathogen.
The exit door of the causative agent from its reservoir may vary depending on its location. Inside the animated and animal reservoirs, the exit doors can be; respiratory, digestive, genito-urinary or skin and mucous membranes.
Once the causative agent leaves its reservoir, it passes to the new host through a transmission route.
The routes of transmission of the causative agents can be direct, through direct physical contact; without physical contact, such as through a sneeze; or indirect, through contaminated items, such as syringes or food.
In order for the causal agent to enter the new host, it needs a gateway. The entry ports are the same as the exit ports, respiratory, digestive, genito-urinary or skin and mucous membranes.
Once the causative agent enters its new host, it will be infected if natural conditions are suitable for the development of the biological agent..
The hosts are humans and animals. Since inanimate beings, although they may contain biological agents, they cannot be affected by them.
The hosts may be susceptible to infection as they do not have sufficient defenses against the pathogen. However, there are body defense mechanisms against toxic agents. These hosts are known as immune. Immunity, which is the host's state of resistance, can be natural or acquired.
Immunity is the state of resistance of the organism against external attacks. The body has defense mechanisms, known as effector systems. The defense mechanism recognizes the components of the pathogen and begins the process of eliminating it.
First, the cells affected by the pathogen are located, and a barrier process is started so that it does not spread. Barrier methods can be mechanical or chemical. The former are physical impediments such as the outer layer of the epidermis.
Chemical impediments form a hostile environment where the pathogen cannot thrive. Some examples of chemical impediments are saliva and sweat, among others.
When inflammation occurs, it is because the pathogen is attacking a tissue, the response of this is inflammation to locate the agent and stop it.
Immunity can be natural or acquired. Natural immunity is one that provides a general barrier and does not need to be stimulated. It can be the skin, mucous membranes and saliva, among others.
Acquired immunity is one that needs external stimuli. This can be active, when it is the body itself that recognizes the pathogen and initiates the protection process.
Another case of acquired immunity is passive, when the body receives other foreign antibodies formed in another host. Passive acquired immunities include medicines and vaccines.
When pathogens move from their reservoir to a host, they can multiply and spread to multiple hosts. Depending on the frequency of contagion and the time between each contagion, different levels of disease can be distinguished.
In the epidemic, the pathogen infects a higher number of hosts than expected. Still, it is limited in time and space. It is a mass phenomenon that exceeds the normal incidence of the pathogen
In this case, the pathogen infects a number of hosts in an unlimited space. It can cross country borders or even continents, but it is limited in time
The number of pathogens multiplies and lengthens in time and space. There are numerous cases for an unlimited period of time. This is when epidemiological surveillance by the corresponding institutions begins..
These institutions need to know in detail the development of the epidemiological chain to stop it and be able to update the population with information on how not to contract the pathogen.
According to the WHO, prevention is based on measures whose objective is to prevent the onset of the disease, put an end to its progress, limit the damage it produces and mitigate its consequences once established.
There is a preventive medicine study conducted by Leavell and Clark. In 1958, these authors postulated that the disease begins with the state of health and that the outcomes that result are the evolution of the disease.
Preventive medicine studies how to prevent disease and promote health and longevity. Leavell and Clark postulated three levels of prevention, primary, secondary and tertiary.
Primary prevention is that which occurs in the phase prior to the development of the disease or prepatogenic phase. At this stage, the host cells have not yet been involved in the process..
It is at this time that the beginning of the epidemiological chain develops and the pathogen moves in the direction of the new host. To prevent diseases in this phase, general health is promoted, with healthy eating and exercise habits.
Secondary prevention develops in the pathogenic phase of the virus. In this phase we are at the point of the epidemiological chain where the host is infected by the pathogen and the host is directly affected..
In this phase is where the incubation period occurs and the changes are recognized by the host as symptoms of disease. As a prevention method, specific protection is used, that is, diagnosing the disease, and starting with measures indicated especially for a type of disease already recognized..
Tertiary prevention is in the recovery phase, in what is known as the post-pathological period; trying to limit the sequelae or starting rehabilitation.
At this level of prevention, an attempt is made to limit the damage caused by the pathogen in the host and the rehabilitation process begins if there is any type of sequelae to lead to a comprehensive recovery..


Yet No Comments